Related Research
In his early days as India’s new prime minister, Narendra Modi has shown remarkable leadership in all sectors, including health, for which he’s articulated his vision to create a Swasth Bharat, a Healthy India. Combined with two major policy windows—the proposed restructuring of the Planning Commission and the report of the 14th Finance Commission expected by the end of the year—the policy reforms under the ruling National Democratic Alliance (NDA)’s mandate of “Universal Health Assurance for All” have the potential to be a game-changer for India’s neglected public health system.
India’s health system has many problems but perhaps the most obvious is its persistently low levels of public financing for health, with often limited health outcomes. With only 1.7 percent of its GDP being spent on health expenditures (including sanitation and nutrition), India spends roughly $15 per person for health each year. As a result, up to 75 percent of health care expenses are borne out of pocket by patients. And given the lack of any mechanism to insure against health risks, much of India’s low-income population has to forego necessary healthcare or is forced into bankruptcy because of the inability to pay when confronted with a severe medical condition.
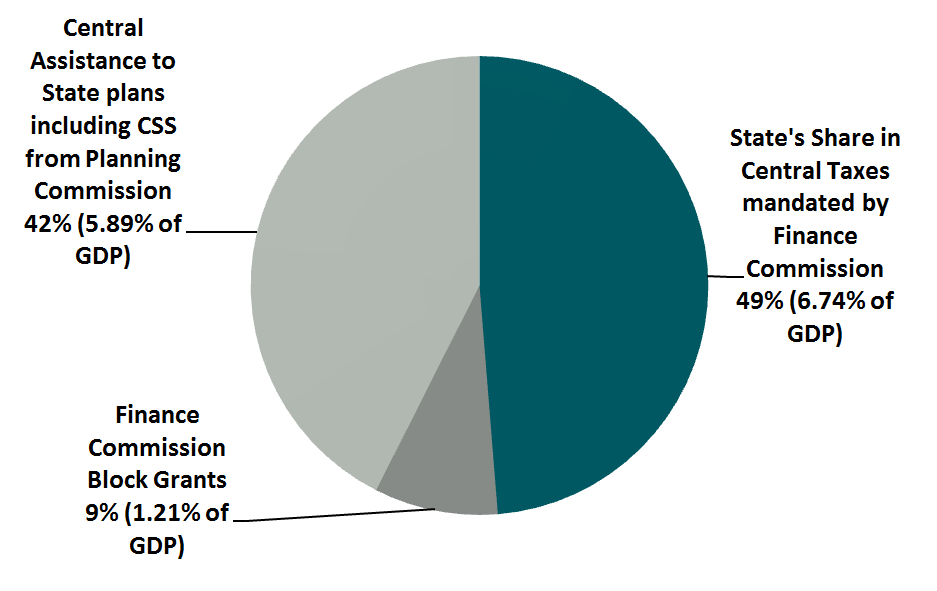
One critical policy lever that could have an impact on Indian public health expenditure and its effects on health outcomes is the financial flows and incentives from central government to states. India’s center-to-state fiscal transfers have occurred through three channels—Finance Commission; Planning Commission; and Centrally Sponsored Schemes—with at least three crucial characteristics (see figure 1):
- Are the allocations based on a formula and objective criteria or not?
- Are there conditionalities associated with those transfers?
- Who does the money go to?
While health is a ‘state’ subject, the central government has exerted significant influence on health financing through the flagship scheme known as the National Rural Health Mission (NRHM) from 2006–07 onwards. NRHM has now been extended to cover urban areas under the National Health Mission (NHM) umbrella. However, a systematic assessment of the impact of the three channels of transfers at the state level has not been attempted until now.
Over the past year, the Center for Global Development and the Center for Policy Research’s Accountability Initiative (in Delhi) have conducted research on intergovernmental fiscal transfers to improve health in India. As an early step we commissioned a background paper that describes and analyzes the myriad of channels and mechanisms of center-to-state fiscal transfers that could affect health outcomes. See a draft of the background paper here.
Building on this background paper, Accountability Initiative and CGD have jointly pursued several areas of research to better assess the consequences and effectiveness of these different channels of funding—between Planning Commission and Finance Commission, within the Finance Commission, and the ‘Centrally Sponsored Schemes’ for health. In December, we are convening a working group to discuss some of our early findings and policy recommendations.
Disclaimer
CGD blog posts reflect the views of the authors, drawing on prior research and experience in their areas of expertise. CGD is a nonpartisan, independent organization and does not take institutional positions.



