Recommended

Event
Making Fragmented Aid Flows Work Better for Health

Blog Post
Financing Outbreak Preparedness: Where Are We and What Next?
The COVID-19 pandemic has exposed the ways in which global pandemic preparedness and response are under-prioritized and under-resourced. But the good news is that today’s shortfalls are finally eliciting global action. US Secretary of State Antony Blinken recently announced the US administration’s intent to “advance the creation of a long-overdue sustainable financing mechanism for health security, so we can leave the world more prepared for future outbreaks than it was for this pandemic” and President Biden reaffirmed the US commitment to advancing global health security in his comments to the G-7. These pledges come on the heels of a new G-20 member-launched independent panel on the future of financing pandemic preparedness and response.
The global case for preventing and containing pandemics in terms of human and economic well-being is self-evident. To date, COVID-19 has claimed the lives of more than 2.5 million people and could cost the global economy US$10.3 trillion over 2020-2021. While the estimated cost of preparedness is only in the tens of billions, the question of how to mobilize adequate resources before outbreaks spread, and how to get the incentives right at all levels, remains.
This idea is not new. As the interim report published by the Independent Panel for Pandemic Preparedness and Response points out, twelve different commissions and panels have examined outbreaks, pandemics, and the International Health Regulations (IHR) during and in the aftermath of the 2009 H1N1 pandemic, the 2014-2016 West Africa Ebola outbreak, and the ongoing COVID-19 pandemic. Most called for scaled-up and sustainable financing for pandemic preparedness and response. Colleagues at the World Bank, CSIS, CFR, Georgetown, NTI, Resolve to Save Lives, and others have also looked at these issues and made recommendations. (And CGD has joined in.)
To get to the next stage, we must understand the current landscape:
Updating our understanding of what constitutes pandemic preparedness and its costs
Over the years, the global community developed ways to define and assess national capacities to prevent, detect, and respond to public health emergencies, including the International Health Regulation-based Joint External Evaluation (JEE) and the Global Health Security Agenda (GHSA). In 2019, the Nuclear Threat Initiative and the Johns Hopkins Bloomberg School of Public Health Center for Health Security also developed the Global Health Security Index to assess and benchmark health security across IHR States Parties. To date, 100/195 countries have undertaken a JEE, and 69 countries have signed onto the GHSA framework.
But over the past year, we’ve seen repeatedly that higher scores on existing measures have not necessarily translated to better preparedness or a successful response to combat a global pandemic. Further, the evolving crisis shows that beyond identifying structures and processes, we need measures that reflect how well preparedness systems perform in the real world. Not desktop exercises, but instead how quickly tests can be turned around, or how completely and accurately deaths are recorded. Former CDC Director Tom Frieden, for example, recently proposed a new goal for early warning and response to guard against the next global health threat, which rests on three numbers “7-1-7.” That is, our aim should be to get to where “every country can identify any new suspected outbreak within seven days of emergence, start to investigate the event within one day and report it then, and mount an effective response – defined by clear, specific benchmarks for different pathogens—within seven days.” Richard Hatchett of CEPI has called for a commitment to compress the timeline for vaccine development to 100 days from genetic sequencing of a novel virus to submission of phase 3 clinical trial data, while the scientist Florian Krammer calls for an uber-CEPI, with a broader mandate and increased funding. Meanwhile, as the pandemic unfolds, our understanding of what preparedness functions are required is evolving. Historically, genomic surveillance has largely been run by academic groups, but the emergence of variants shows how this, and other kinds of surveillance capabilities, need to be widespread, standardized, and embedded (and funded) as part of national preparedness activities.
We need measures that reflect how well preparedness systems perform in the real world
Each of these expanded capabilities has a price tag attached that needs to be assessed, and some minimum standards should be spelled out clearly. To date, estimates of the full cost of pandemic preparedness have varied widely. At the high end, McKinsey & Company recently estimated that preparedness will cost US$70-120 billion over the next two years, and an additional US$20-40 billion annually after that (though their methods are not fully detailed in the public domain). A 2016 National Academy of Medicine (NAM) Commission calculated the cost of preparedness at US$4.5 billion per year. Their figure is based on the estimated cost of upgrading public health systems, the cost of enhancing WHO’s pandemic prevention and response capabilities, and proposed incremental investment in research and development. And a 2012 World Bank report projected the annual cost of preparedness to be US$1.9-3.4 billion per year.
But while the estimated costs of pandemic preparedness are probably out of date and may vary, requirements are evidently a sliver of the cost of response and recovery.
Even the highest cost assessments associated with preparedness are dwarfed by projected costs of response and recovery in the wake of a major disease outbreak. We can look to past health emergencies for estimates of the economic toll (Figure 1). For instance, the productivity loss from the 2003 SARS epidemic is estimated at US$40 billion. The total cost of the 2009 H1N1 influenza pandemic is estimated at anywhere from US$45-55 billion. And the economic and social impact of the West Africa Ebola outbreak in 2014-2016 may have cost as much as US$53 billion.
Figure 1. Estimated costs of past health emergencies
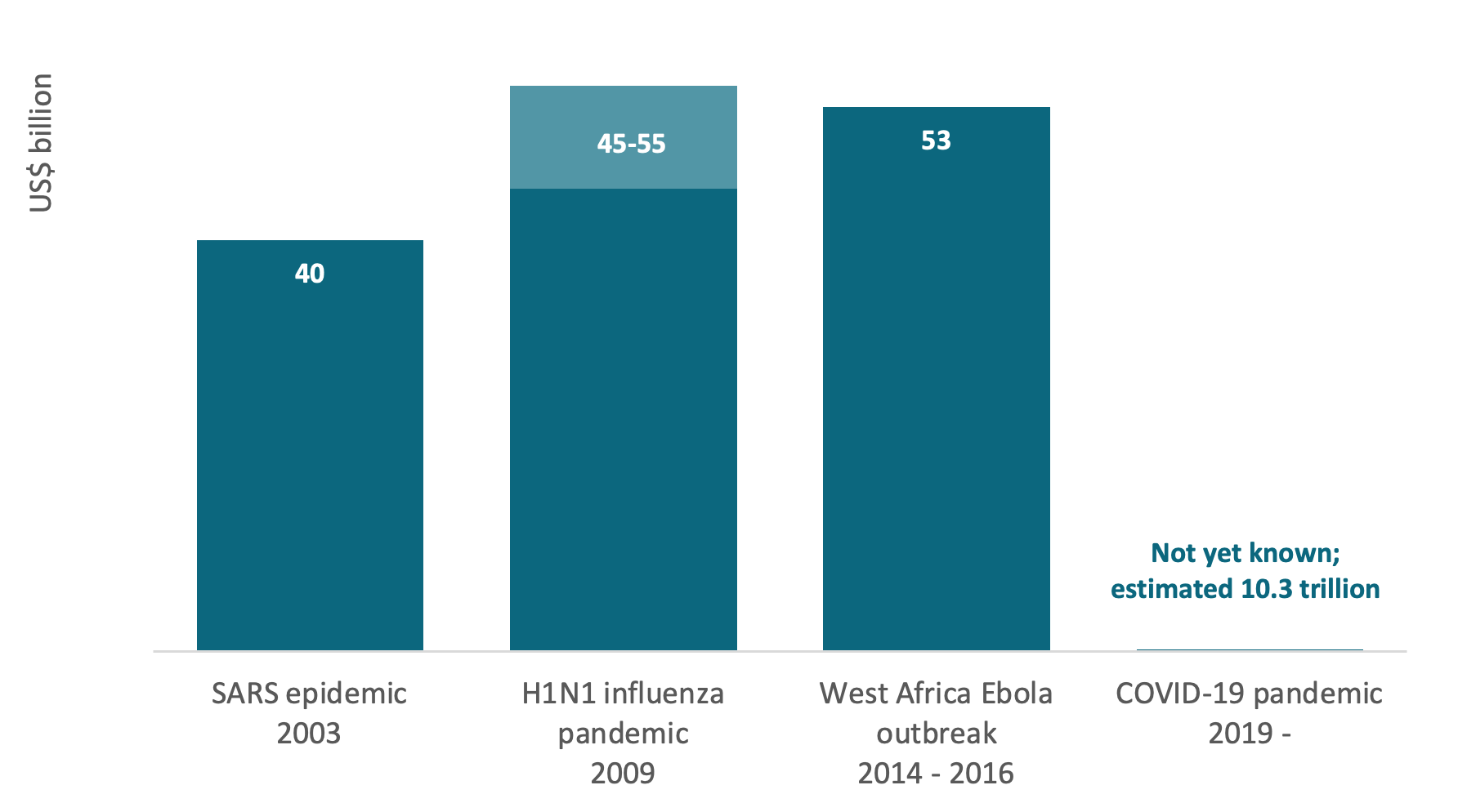
*Costs are calculated as follows: SARS – productivity loss; H1N1 – total cost; Ebola – economic and social impact; COVID-19 – forgone output.
Previous epidemics were much less devastating at the global level when compared to what we are enduring now—and will continue to face in the aftermath of the COVID-19 pandemic. Some have estimated the total of forgone output (goods and services the world could have produced) due to the COVID-19 pandemic could amount to US$10.3 trillion. The same McKinsey paper puts the cost of COVID-19 response and recovery at US$9-33 trillion, while the Global Preparedness Monitoring Board estimates the response will require US$11 trillion in direct funding and cost US$10 trillion in future loss of earnings.
But also: the lowest estimates of financial needs for preparedness vastly exceed current spending on public health in general.
By OECD countries
A small fraction (2.8 percent) of domestic health spending in OECD countries goes toward prevention (that includes public health and preparedness), and an even smaller proportion is allocated to disease detection and immunization. Average preventive care spending by OECD governments is low as a share of total funding, and has stayed low over time (Figure 2). In the United States, according to the Trust for America’s Health, spending on public health has been decreasing since 2000.
Around the world, health spending is concentrated in clinical care for individuals and acute care for injury and illness—not in preventive measures and preparedness. As Harold Pollack writes, despite spending US$3.8 trillion on medical care in 2019, the US was not prepared to produce masks that could be manufactured for less than a dollar each. Public health is not part of universal health coverage entitlements and is frequently delegated—often without explicit funding or standards—to states, provinces, and municipalities. As such, there are few incentives to assure minimum levels of preparedness (little routine use, little accountability), and as a result, preparedness and response is often neglected or only "on the books"– memos and guidance at the federal or central level, with little action at the subnational level.
Figure 2. Average preventive care spending by government in OECD countries
For countries with available data
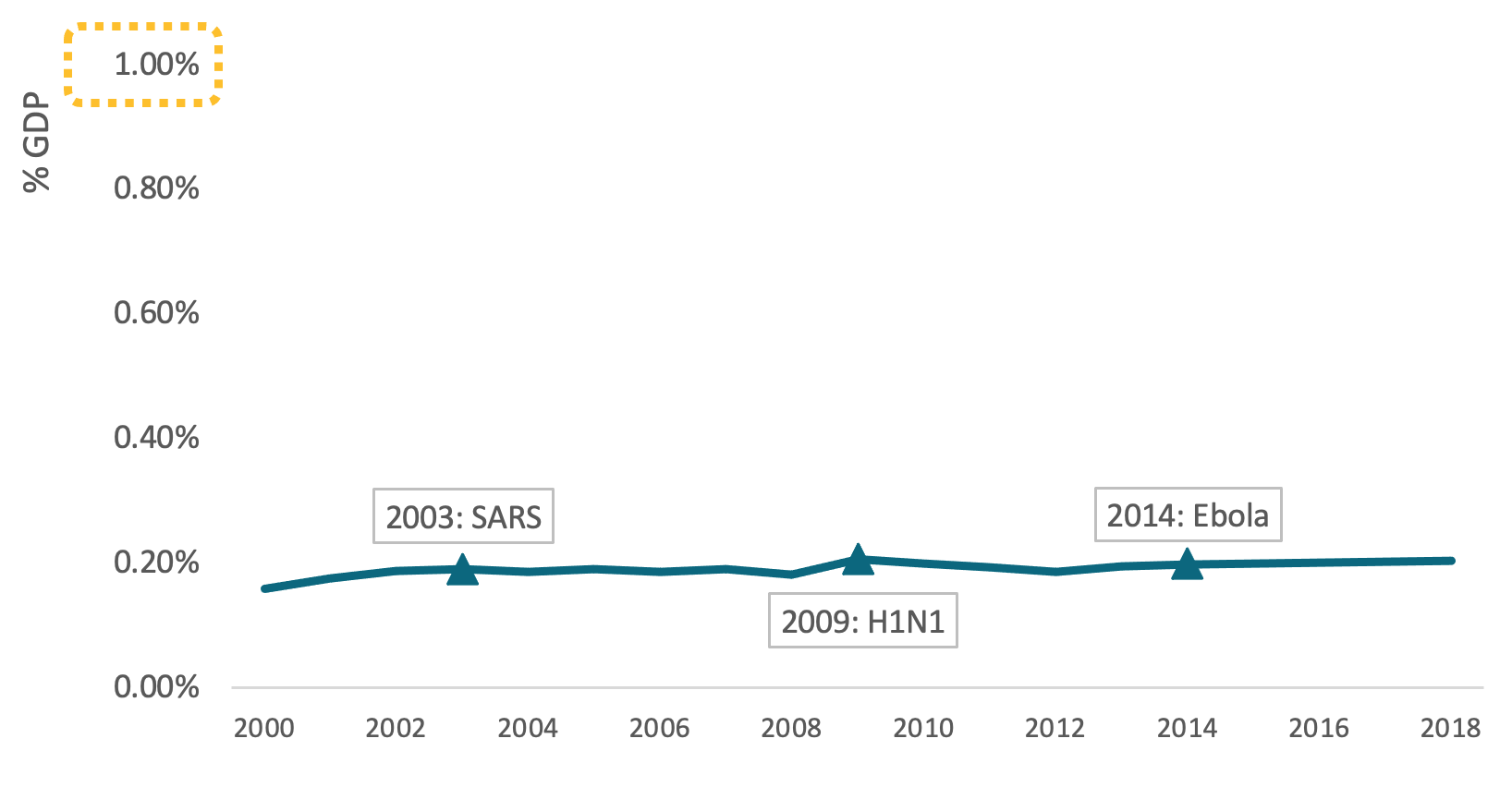
Data source: OECD
By low- and middle-income countries
Domestic spending on preparedness per se in low- and middle-income countries is not well documented, but country-specific costing studies of the IHR indicate requirements comprise a significant share of per capita public spending on health (e.g., in Nigeria). But overall government spending on health per capita in low- and middle-income countries is a small fraction of what is spent in high income countries, and ranges between US$35-85 per person per year. And the opportunity costs of spending on preparedness versus other uses of health spending are potentially large, providing an additional explanation of why this kind of spend is not often prioritized by governments. As the global community considers financing options, it must also examine where concessional financing will be needed to support greater low- and middle-income country investment.
In international assistance
Epidemic and pandemic preparedness and response spending as part of global health aid has increased after health crises historically, but (even then) remained a modest proportion of development assistance for health. During the West Africa Ebola outbreak, epidemic and pandemic preparedness and response increased to 16 percent of global health aid in 2015, and then quickly fell again in 2017 to seven percent. In 2019, Tom Bollyky and co-authors from IHME estimated that pandemic preparedness made up just 0.9 percent of global health aid (Figure 3).
Figure 3. Development Assistance for Health
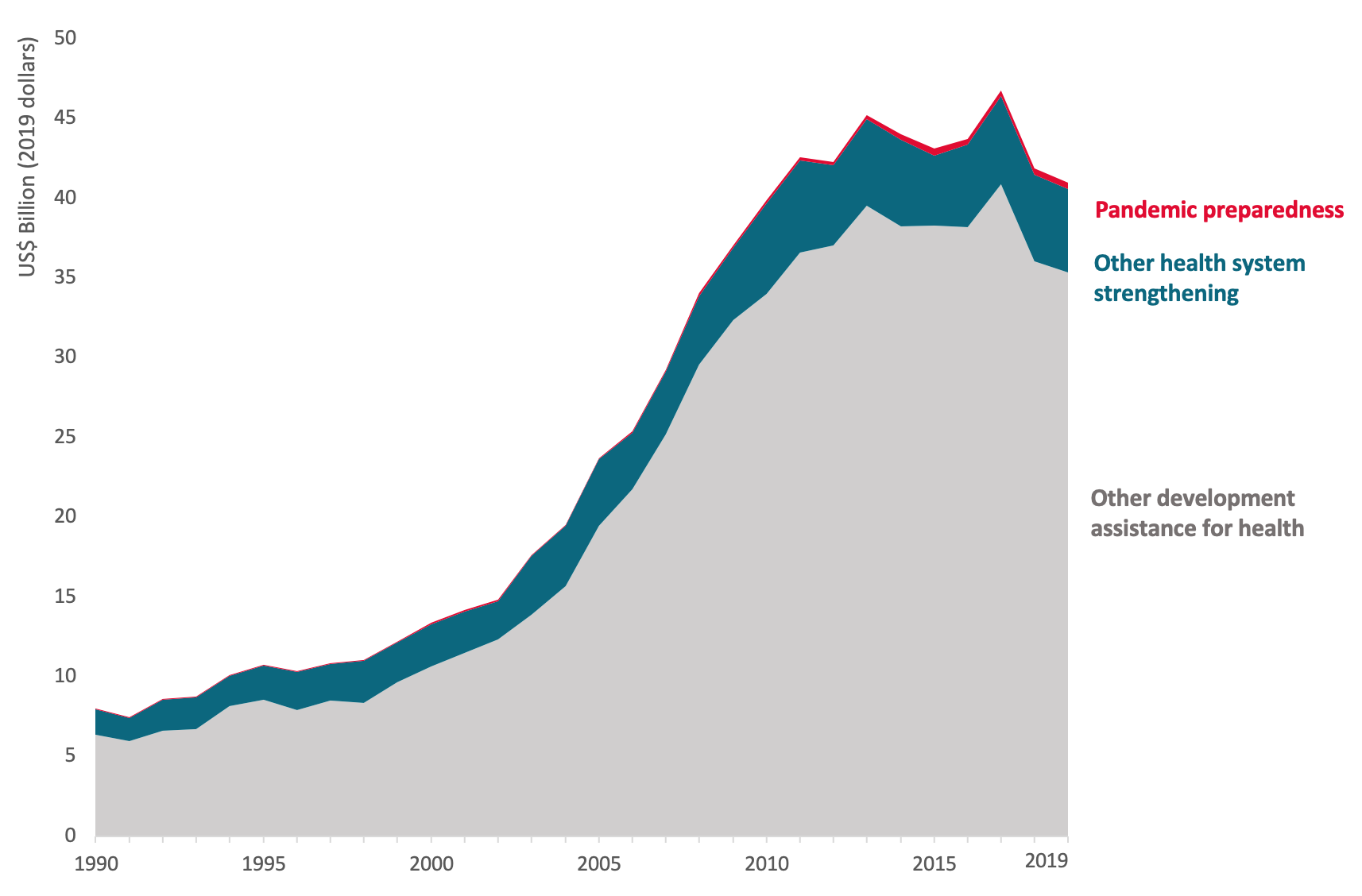
Graph modeled on Bollyky and Patrick (2020)
Data source: Institute for Health Metrics and Evaluation
We also know, thanks to Rebecca Katz and co-authors’ efforts to track the flow of funds in this area, that existing spending on global health security is largely directed to immunization and emergency response operations (see Figure 4). The Bill & Melinda Gates Foundation and the US Government (via USAID and others) are the top funders of global health security over 2014-2021.
Figure 4. Tracking the Flow of Funds in Global Health Security
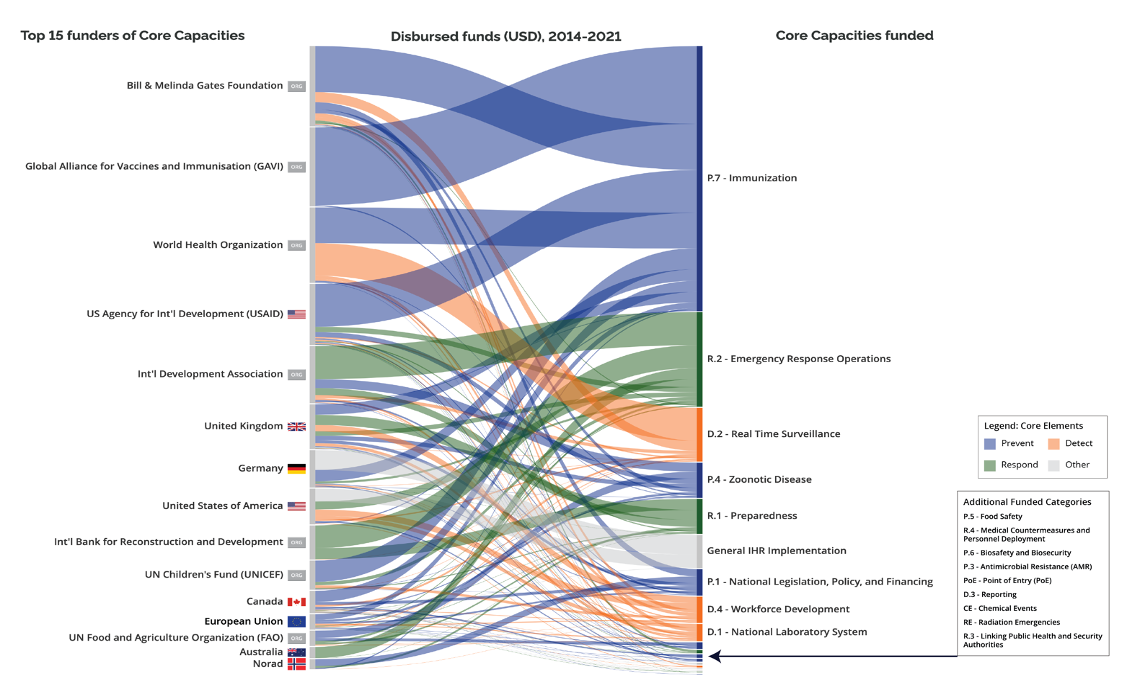
Source: Data up to date through January 2021; generation of data based on Katz, R; Graeden, E; Kerr, J; Eaneff, S. “Tracking the Flow of Funds in Global Health Security.” EcoHealth (2019) 16:298-305.
And – as is now well-known – the financing situation of the WHO in particular is lamentable: Member States’ decisions to limit assessed contributions have kept the WHO under-powered and under-resourced, undermining the organization’s ability to do its job effectively. COVID-19 has highlighted this chronic underfunding of WHO. Nearly 80 percent of the WHO budget is voluntary and highly earmarked, hindering WHO’s operations and, according to its own assessments, precluding holistic preparedness efforts.
At the global level, financing of pandemic preparedness and response is also characterized by its small scale and fragmentation. Multiple international programs, initiatives, and institutions emerged in the aftermath of the West Africa Ebola outbreak, most were small in scale, related to response, and overall, inadequately funded. There is the successful example of the Coalition for Epidemic Preparedness Innovations (CEPI) – which, as of November 2020, had raised US$1.3 billion in support of COVID-19 vaccine research and development but needed US$800 million in additional funds, but there is also the cautionary tale of the now defunct World Bank-based Pandemic Emergency Financing Facility (PEF).
The World Bank hosts a number of initiatives to finance emergency response – the newest is the Health Emergency Preparedness and Response Multi-Donor Fund (HEPRTF), announced in April 2020, which provides financing to low-income countries and to countries with low health emergency preparedness and response scores. On preparedness, with external philanthropy, the World Bank has also supported technical assistance for preparedness via REDISSE and uses its regular lending windows for such investments. However, historic country demand for World Bank lending in these areas has been minimal.
More broadly, we see disease-specific financing of cross-cutting preparedness functions like mortality recording, surveillance, and laboratory, as well as emergency procurement. There are examples of COVID-19 pivots by the vertical funds that are laudable – Gavi and collaborators’ work to create COVAX, the COVID-19 vaccine procurement platform, and the Global Fund’s flexible grants and information on sourcing and management of COVID-19 related health products, for example, have been important in the response to date.
However, fragmented financing for preparedness and response can lead to duplication (multiple global windows of procurement for vaccines, PPE, tests, etc.; siloed surveillance or lab systems) and does at least seem inefficient when assessed against the overall performance of some of these systems in countries that have been big recipients of disease-specific monies. Mortality reporting is perhaps the most egregious example with WHO recently noting that 40% of the world's deaths go unreported, mostly in low-income countries, and that cause of death is unavailable in 92% of deaths in these same settings.
What next?
While the economic case is clear and experts are unanimous on the need for greater finance, the public good nature of some the actions, competing demands for scarce public monies in LMICs, and reliance on small-scale aid and philanthropy as sources of finance have meant chronic underfunding in the past. Even new international mechanisms established since the onset of COVID-19 remain underfunded – as of January, 2021, ACT-A, the mechanism to finance vaccines and other needed products to battle COVID-19 faces a financing gap of US27.2 billion.
Immediate funding issues need to be addressed first, but as global leaders consider what comes next, we also need a clearer definition of what constitutes the minimum acceptable standard of preparedness, a closer look at getting the sizing, organization, and incentives of financing right at both national and global levels, and, of course, dedicated and sustained financing sources.
There are new developments to consider – the HERA Incubator launched last month, a European Community version of BARDA and a move to create a new class of public expenditure in the US Health Defense Operations. The World Bank is looking to host an early replenishment of its main concessional window (IDA 20) later this year, perhaps representing another opportunity to prioritize preparedness. The last replenishment, IDA19, featured a policy paper on pandemic preparedness but no major actions beyond a suggestion from donors that the Bank engage in dialogue with its borrowers around the issues. And other proposals are circulating as well: ideas from the Pandemic Action Network include our work with colleagues at CSIS and NTI on a Global Health Security Challenge Fund, and the Independent Panel for Pandemic Preparedness and Response may recommend new modalities, among others.
Stay tuned, and as always we welcome your feedback and public commentary.
Topics
DISCLAIMER & PERMISSIONS
CGD's publications reflect the views of the authors, drawing on prior research and experience in their areas of expertise. CGD is a nonpartisan, independent organization and does not take institutional positions. You may use and disseminate CGD's publications under these conditions.


