Recommended

Blog Post
How a Pandemic FIF Should Be Different

Blog Post
Can You Spare .001% For the World’s Pandemic Fund?

On November 13th, 2022, the creation of a new Pandemic Fund, hosted by the World Bank, was announced. The goal of the Pandemic Fund is to provide a currently missing dedicated stream of additional, long-term funding to support low- and middle-income countries (LMICs) to support and reinforce pandemic preparedness and response (PPR) capacities. Its mandate is ambitious: to successfully prevent, prepare and respond to emerging pathogens. This will require true collective action, and implementation of decisive and ambitious policies in as many parts of the globe as possible, since the strength of PPR is, in part, the sum total of the performance of all national systems.
While much of the details of how the Pandemic Fund will operate is still being discussed, we do know it will release its first call for proposals in early February, which will be an opportunity to pilot approaches and learn. In this blog, we ask how can it best fund discrete country-specific projects to effectively produce the true global public good of global health security? On what basis will the newly appointed Technical Advisory Panel evaluate projects? In particular, we identify three challenges that we think will make the definition of priorities complex: the vastness of the PPR agenda as well as the paucity of evidence; the need to value projects from both a national and global perspective; and the need to match the source of the funding with appropriate projects.
The decision space is enormous and under-researched
There is not one definition of what may fall within the scope of PPR. A useful definition from McKinsey is organised around the following capabilities—which can be further broken down into a high number of interventions ranging from genomic surveillance to strengthening vaccine manufacturing capacities.
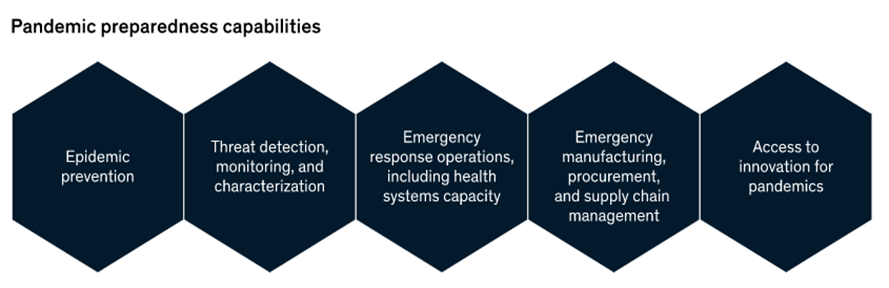
Source: McKinsey
Other experts have characterised a vision of PPR that builds on core health systems capabilities and universal health coverage; which would further expand the scope into a wide variety of health system strengthening initiatives. In addition to the decision-space being vast, the evidence base surrounding those interventions isn’t yet well developed to readily support in-country investments. Just on costing, a recent literature review found ten studies and argues for improved methods, greater interpretation, and comparison across studies. On cost-effectiveness of outbreak response, a review also found similarly few studies. The methods for evaluating PPR are also not well established, partly due to lack of data on cost or effectiveness of interventions, uncertainty in the timing and nature of the threat, as well as uncertainty in the future economic and health system context (e.g., vaccine manufacturing capacities, health systems constraints).
The need to appraise interventions from a national and global perspective
Unlike other areas of global health, pandemic preparedness is truly a global public good that benefits everyone. So here the Fund needs to carefully consider who benefits from greater PPR, and how those benefits materialise. For instance, the benefits of the Global Fund’s vector control in malaria are straightforward: the intention is to limit the spread of malaria for the communities that receive the interventions. Whereas for the Pandemic Fund, we see two types of benefits arising from individual PPR projects:
- Direct benefits to recipient co-investor countries—in terms of health systems strengthening (e.g., stronger laboratory capacity, disease surveillance) and of greater health security (e.g., through controlled epidemics, averted lockdowns or disruptions to the economy).
- Indirect benefits globally in terms of greater health security (same as above) that accrue to all other countries.
The presence of such externalities creates a complexity about how to, in theory, define value and to whom. Some interventions may be good value for money at the global level but have poor value for money for the recipient country; for instance, disease surveillance for a virus that causes low morbidity in a given country may be beneficial globally but not so for the recipient country. On the other hand, planning for surge capacities to maintain essential service provision may be beneficial to recipient countries, but less so internationally. How will the Fund consider or estimate those externalities? And how will it prioritise between projects that impact countries and regions differentially? There is no quick-fix, technical solution that can be deployed easily. The Fund has launched a Working Group to consider criteria for resource allocation, but it has not yet reported back. It is worth noting that in the design of its Governance mechanism, the Fund is seeking to ensure that balanced perspectives from LMICs and high-income countries (HICs) drive the operation of the Fund. The Governing board has equal representation of donors and country co-investors (from LMICs), as well as two Civil Society Organisations seats. But without an appropriate and explicit prioritisation framework that considers both national and global benefits, it is unclear how this governance process will be empowered to take difficult but evidence-informed, criteria-based decisions.
Who pays and why does it matter?
At the moment, the Fund draws resources from voluntary contributions from countries and philanthropies, and will leverage domestic funding from countries through the International Development Association (IDA) mechanism. The target for the Pandemic Fund is to mobilise US$10.5 billion per year to be able to achieve its stated goals. So far, the Pandemic Fund tracker shows that only 13 percent of its target has been raised (US$1.6 billion announced from 26 donors; 23 countries and three philanthropic organisations). The two largest donors, the US and EU, both providing US$450 million, have categorised their contributions as non-Overseas Development Assistance (ODA).
Despite the obvious benefits of PPR for all, we need to think about whether such benefits tend to accrue to specific groups of countries and how this links to who pays for the Fund. If we take the example of COVID-19, one may argue that in absolute monetary terms (one metric by which benefits can be -incompletely- measured), the lion’s share of the total cost of the pandemic fell on high- and upper-middle income nations (given the sheer size of the GDP of such countries compared to lower- and lower-middle-income countries (L&LMICs)). In simple terms, if COVID-19 had been averted through PPR interventions, then higher income nations would have reaped the greatest benefits in economic terms. In the US alone, one estimate puts the cost of the pandemic at a staggering US$16 trillion. One preliminary analysis from Imperial College London and commissioned by the G20 High Level Independent Panel makes a similar point: the group looked at the return on investment (ROI) for hypothetical PPR interventions, and showed that it varied between US$34 to US$1,703 for a COVID-19-type of pandemic; with higher ROIs in higher income nations.
These benefits falling on higher income nations are particularly important to consider if the Fund intends to incentivise the use of L&LMIC domestic resources (or loans) for PPR, or where the Fund raises money that is primarily ODA; because this may reduce funding elsewhere: either from other domestic priorities or other L&LMIC global priorities, and this displacement will have opportunity costs. The Fund Board may therefore wish to formally adopt an additionality policy to describe how it will manage this risk.
Conclusions and policy recommendations
Three years on, COVID-19 continues to wreak havoc in many parts of the world. The value of averting a future pandemic and better equip countries to effectively respond is undeniable—which is what makes the work of the Pandemic Fund so important, yet so complex. Ensuring that the scarce funding managed by the Fund goes towards producing the most impact should be central to the next months. We make three recommendations:
- The Fund consults stakeholders on priority areas in the PPR space (especially voices from LMICs) to understand the scope of work and its comparative advantage compared to other global health initiatives. Within this it should not lose sight of global public goods and supporting the development of much needed evidence base around PPR interventions. This could include working with the World Health Organization and academia to maintain a register of research topics for areas where it is not able to prioritise effectively due to lack of evidence.
- The Fund develops a priority setting framework that adequately considers projects from a domestic and global perspective. There may not be an easy analytical solution to resolving different valuation of projects from different perspectives. One solution is to consider lessons from the Health Technology Assessment field: i.e. setting clear criteria, collating evidence on each criteria, having a deliberative committee that considers all reasonable values and perspectives, making explicit decisions, and reviewing regularly.
- The Board of the Fund may wish to set out an explicit additionality policy. Due to the differential impact of projects on different countries, the Fund may wish to consider if some projects are more suitable for ODA or non-ODA funding for instance, and to what extent co-financing of domestic resources is appropriate.
Topics
DISCLAIMER & PERMISSIONS
CGD's publications reflect the views of the authors, drawing on prior research and experience in their areas of expertise. CGD is a nonpartisan, independent organization and does not take institutional positions. You may use and disseminate CGD's publications under these conditions.
Thumbnail image by: Adobe Stock


