Recommended

This blog is part of a series focused on the UK’s recruitment of foreign-trained health workers. The first blog details the amount of money the UK’s National Health Service (NHS) has saved by recruiting foreign-trained health workers. This second blog examines whether this saving is offset by foreign aid contributions to health systems strengthening (HSS) and human resources for health (HRH) in countries of origin. Regardless of the method chosen, calculations suggest the financial benefits to the UK dwarf the amount of money spent abroad.
The UK’s All Party Parliamentary Group (APPG) on Global Health & Security—supported by Global Health Partnerships (formerly THET) and the Center for Global Development (CGD)—has conducted an inquiry into the impact of international recruitment and health worker mobility. One key question stood out: how much has the UK saved in training costs by recruiting foreign-trained health workers?
As of June 2025, the NHS employed 218,727 non-British doctors, nurses, health visitors, and midwives (~35 percent of the total). Training them domestically would have cost £14 billion, a massive saving for the cash-strapped NHS.
Even more strikingly, between mid-2024 and mid-2025, the stock of foreign-trained health workers in the NHS increased by 7,719. The UK therefore saved £1.1 billion in the last year alone from not having to pay to train these health workers.
The inquiry’s report—launched today—focuses on the notion of “proportionate co-investment”. It argues that countries of destination such as the UK should be spending a portion of these averted training costs on HSS and HRH interventions in countries of origin, to offset the loss of human capital.
This blog therefore compares this £1.1 billion saving with the UK’s current aid spending on HSS, using two different methodologies, to ascertain whether this offsetting is happening in practice. Because the health workforce is a core building block of HSS—and typically funded under that heading—this provides a rough benchmark for assessing the gap (Figure 1). The findings are striking: using the most conservative estimate, the UK saves five times what they spend in countries of origin.
Figure 1. The six essential building blocks of the health system needed to improve outcomes
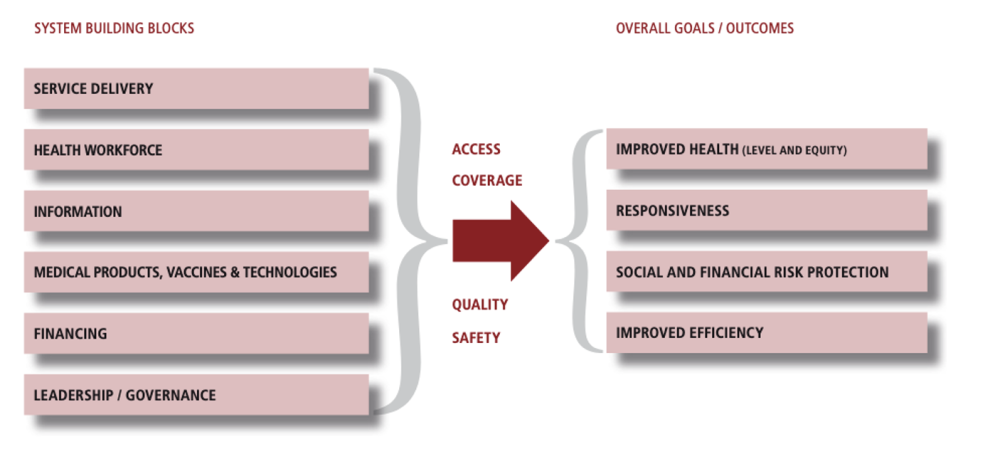
Source: WHO (2007)
Assessing the gap in averted training costs
Methodology 1: Spending on HSS
In 2025, the UK’s total contribution to “development assistance for health” (DAH) was £1.3 billion. Of this, £232 million went to HSS and sector-wide approaches (SWAPs, investments which support a single, national, health policy rather than fragmented projects). This HSS funding goes towards strengthening the core health system building blocks—all of which are needed to improve health outcomes—including health workforce investments.
Recognising the importance of HSS for global health security and universal health coverage (UHC), the UK has historically emphasised the centrality of these investments in their global health policy (e.g., see their 2023 Global Health Framework). Examples of the UK’s efforts include a programme for training and mentorship on emergency obstetric and newborn care in Kenya, and a Department for Health and Social Care (DHSC)-supported Health Partnerships initiative to address workforce shortages and expand training and management capacity across Africa.
Going purely on strategy documents, the UK’s commitment to HSS is clear. However, if we take HSS financing as a proxy for HRH contributions, the UK’s averted training cost savings are nearly five times larger than its expenditure on HRH. Given HRH is a component of HSS, this is likely to be a conservative estimate of how much the UK benefits.
Methodology 2: Spending on HRH
We can also estimate how much money is spent on HRH using global data. Estimates indicate that, in 2020, only 7 percent of global health spending went towards HRH; a peak during COVID. Since the 2025 aid cuts, the total amount of DAH, and the amount contributed towards HRH, is now lower (e.g., UK DAH has decreased from US$3.43 billion in 2023 to US$1.76 billion in 2025).
A crude calculation based on this global estimate would mean that the UK contributed £91 million towards HRH in 2025. This is roughly twelve times lower than its saved training costs. This means that for every £1 of aid invested in HRH, the UK saved about £12 in averted training costs.
This means that for every £1 of aid invested in HRH, the UK saved about £12 in averted training costs.
Whether we use the more conservative estimate based on the UK’s HSS spend, or the one based on the global data, this gap matters. It underscores the scale of benefit the UK derives from international recruitment and strengthens the case for “proportionate co-investment” in countries of origin.
The case for “proportionate co-investment”
Redirecting savings from training costs into HRH and HSS in countries of origin with the most understaffed and fragile health systems would be affordable, fair, and strategically smart. It would help sustain the very workforce pipelines the UK relies on—pipelines which have been a core component of the NHS since its inception in 1948. The UK’s reliance on international recruitment is structural, not temporary, and the system-level costs borne by countries of origin cannot be overlooked.
In reality, the recruitment of foreign-trained health workers will remain a central feature in the NHS, regardless of domestic reform ambitions outlined in its 10-Year Plan. A more sustainable path, therefore, requires strengthening the UK’s domestic workforce and the global health workforce it draws from. “Proportionate co-investment” is not simply a moral argument; it is a strategic one. A well-financed, adequately staffed, and resilient global health workforce underpins health security and resilience, thus benefiting the UK as much as partner countries.
Outstanding questions
This blog raises two outstanding questions, which, along with colleagues at the World Bank, we are actively working on addressing. First, how much should we align where we spend our HRH investments and where we recruit from? By and large, the UK recruits from lower-middle- and middle-income countries—the top three countries of origin for nurses are India, Philippines, and Nigeria. These countries may not need HRH support as much as other lower-income countries. Across lower-income countries, the implicit training subsidy that the UK receives is worth around half of all the foreign aid provided to those countries for health over the most recent decade for which data is available (Figure 2).
Figure 2. The UK receives large training subsidies from lower-middle-income countries
Sources: OECD CRS, 2014-2023 (health aid data) and the NHS (workforce data).
Note: Number of nurses and doctors multiplied by average training costs: £22,589 for nurses and £120,693 for doctors (weighted average for consultants and GPs).
Second, if UK stakeholders agree to increase HRH investments, what modality should they choose in an era of aid cuts? DAH has declined from a relatively stable US$50 billion per year in the run up to COVID-19, to an estimated US$38.4 billion in 2025, following the abrupt shutdown of USAID operations in 2025, and substantial budget cuts by the UK’s Foreign Commonwealth and Development Office (FCDO) and other European donors. Indeed, just last week, the UK cut its flagship HRH investment in low- and middle-income countries.
Given these shocks to the aid environment and this era of fiscal uncertainty, increasing HRH investments through bilateral aid seems unlikely. Therefore, it is likely that countries of destination will need to use modalities beyond aid to channel their “proportionate co-investment”. This is the subject of future work by CGD and the World Bank, due to be launched on the sidelines of the World Health Assembly on May 20.
The mobility of health workers is going to increase. To ensure this mobility is ethical and sustainable, investments in HRH and HSS must increase alongside it.
CGD and the World Bank will be hosting a discussion on this topic at the World Health Assembly in Geneva on May 20; and releasing two research papers on modalities to manage health worker mobility and channel HRH financing. To learn more and contribute, please contact Anastassia Demeshko ([email protected]).
Thank you to Lee Crawfurd for his contributions and Figure 2.
Topics
DISCLAIMER & PERMISSIONS
CGD's publications reflect the views of the authors, drawing on prior research and experience in their areas of expertise. CGD is a nonpartisan, independent organization and does not take institutional positions. You may use and disseminate CGD's publications under these conditions.
Thumbnail image by: 098690876



