It is likely that never before in human history have so many been infected so rapidly by an emerging virus as have been with the Omicron variant of COVID-19. And the economic impact of the pandemic over 2020-21 was surely the most damaging ever in terms of absolute dollars of cost: the $10 trillion—and growing—price tag is approximately twice the value of total global GDP at the time of the 1918 flu.
But the reaction to COVID-19 has also been record-breaking. The policy response in many wealthy countries was unprecedented in scale and ambition, protecting lives and livelihoods with public health measures and expanded safety nets. Tragically, it was far smaller in many developing countries, which could not afford to be as generous. Today we release a paper that reports on the development and rollout of COVID-19 vaccines in historical perspective, and it suggests a similar pattern of unparalleled, but still deeply inequitable, progress.
The development process for COVID-19 vaccines was the fastest ever
Never have so many people been vaccinated in one year against a single disease than were vaccinated against COVID-19 in 2021, and never has a global vaccine rollout covered such a large percentage of the population so quickly. For previous vaccines for which we have data, the average period between microbe isolation and vaccine development was 48 years, with a record of about four years. The average time between vaccine development and 40 percent coverage was 42 years, with a record of 14 years for rotavirus. For COVID-19, the period between microbe isolation and vaccine development was less than a year, and between vaccine development and 40 percent coverage just 11 months. It is also worth emphasizing that the reference coverage group for most of the vaccines is children, whereas for COVID-19 we use the total population. This means that the absolute number of vaccinations given is magnitudes larger in the case of COVID-19 than in any previous vaccination program—about 22 times the size of the annual global measles vaccination effort, for example.
Never have so many people been vaccinated in one year against a single disease than were vaccinated against COVID-19 in 2021, and never has a global vaccine rollout covered such a large percentage of the population so quickly.
The figure below shows the speed of rollout of COVID-19 vaccines in 2020 by country income group compared to the first three years of rollout data for vaccines against diseases including polio, tetanus, measles, HPV, and rotavirus. COVID-19 vaccination programs have been dramatically faster to expand than previous programs, and remarkably fast in middle-income countries as well: high- and middle-income countries reached 20 percent coverage rates separated by months, not the years that separated them in previous vaccination rollouts.
Figure 1.
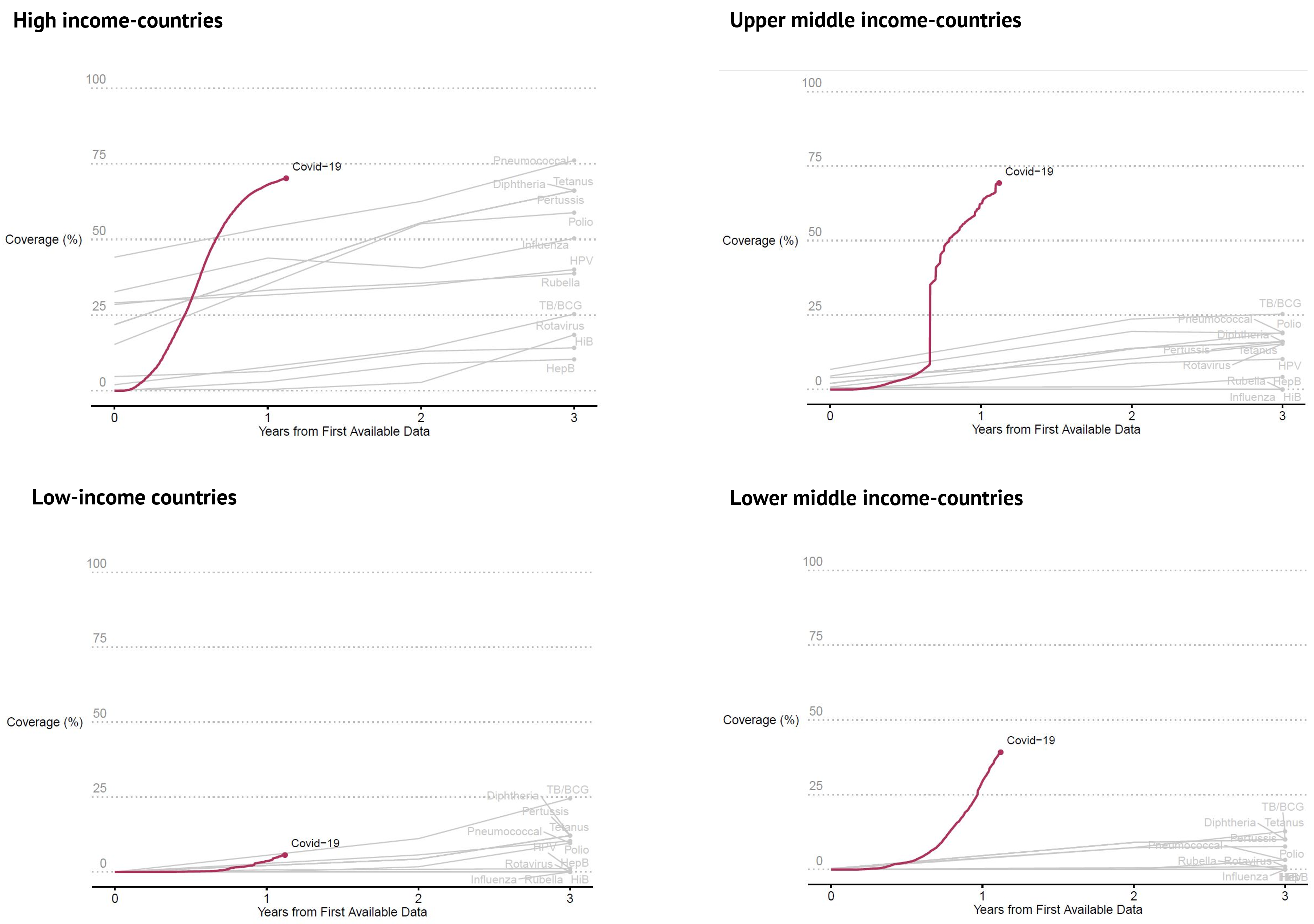
The situation in low-income countries represents the exception
For the world’s poorest economies—home to 9 percent of the world’s population—the first year of rollout was slower than we have seen for some previous vaccination efforts, and it lags very far behind richer countries. On a regional basis, only 6.4 percent of the population in sub-Saharan Africa have been fully vaccinated, whereas more than 58 percent are fully immunized in the OECD countries.
The global pace of vaccination progress is reason for hope, the yawning inequity is reason for urgent action
UNICEF and its Access to Covid-19 Technologies Accelerator partners estimate that only a very modest additional $1.3 billion is needed to increase the pace of vaccination delivery in the lowest-coverage countries. COVAX requires an additional $6 billion to extend coverage and prepare for contingencies such as boosters or new vaccines in case of future, more problematic variants. The rest of ACT-A—which finances tests and treatments for low-income countries—also has a 2022 ask of around $12 billion. These amounts are budget dust for high-income country donors, a sliver of the economic impact of COVID-19 and an excellent investment to avoid prolonging the pandemic.
While there are reasons to hope that COVID-19 will cease to be a public health emergency in the near future, and to acknowledge that low-income countries have experienced lower excess deaths due to age structure, higher vaccination coverage is urgently needed to prepare for downside risks and to fully protect vulnerable populations. Donors: make it months, not years, for low-income countries to reach the necessary vaccination coverage as well.
Topics
DISCLAIMER & PERMISSIONS
CGD's publications reflect the views of the authors, drawing on prior research and experience in their areas of expertise. CGD is a nonpartisan, independent organization and does not take institutional positions. You may use and disseminate CGD's publications under these conditions.


