Recommended

To celebrate World Health Day and the World Health Organization’s 75th anniversary, we‘ve taken the opportunity to focus on this important institution and its essential role in using evidence and knowledge to shape health policies around the world. The COVID-19 pandemic demonstrated the need for an agile, smart, and evidence-based WHO. While Dr Tedros continues his efforts to move reforms ahead in a challenging political environment, we hope he will assure that the WHO is set up to deliver science, knowledge, and evidence—which are ever evolving—to member states and the world at large.
In this blog, we make the case that WHO should shift away from disease siloes and reorganize to streamline the cross-cutting functions that it delivers to member countries. The WHO has an opportunity to streamline its functions along the continuum of science practice—from registering clinical trials and aggregating scientific research and ultimately to evidence synthesis and health technology assessment (HTA) for informing policy recommendations—across the organization.
Science, knowledge, and evidence cut across disease control priorities
The natural tendency of medical professionals is to use a biomedical, clinical, and medical specialty lens (pediatrics, obstetrics, kidneys, heart, chronic disease, infectious disease) as the overarching classification to managing and running health organizations. This biomedical approach has its merits for clinical care, but more and more research has shown the need for greater integration and coordination.
But WHO is not an organization that delivers clinical care, and as such, it should not default to the biomedical or clinical construct. WHO is largely focused on norms and standard-setting, policy advice, technical assistance, and capacity building with member countries. Within the constellation of global health agencies, WHO’s comparative advantage is not in disbursing funding (as is the case with the Global Fund or the World Bank, for example) or in delivering services (e.g. governments themselves or USAID’s private contractors).
Rather, WHO’s core mission is the delivery of the key global public good of science, knowledge, evidence, and data, which cuts across diseases. If we agree on WHO’s core mission, then the question is whether WHO is organized in a way that drives policy and programmatic recommendations, based on ever-evolving science, knowledge, evidence, and data?
The current WHO organigram as of January 1, 2023 shows an array of boxes and siloes. For example, surveillance of antimicrobial resistance (AMR) is under its own box, while intelligence and surveillance systems and data and analytics are in separate boxes. Life-course approaches are segregated from disease-specific approaches under universal health coverage, which are further fragmented from the WHO emergency preparedness boxes.
Yet the functions and types of services that WHO delivers across diseases are shared, including setting guidelines and norms, engaging in policy dialogue, and delivering technical assistance and capacity-building.
The organigram is one of the most important management tools available for ensuring agility and nimbleness, because the siloes created by a chart can hinder the sharing and coordination of resources that might otherwise be possible under a less “boxy” chart. Having fewer boxes can potentially minimize silos and the fragmentation that hinder resource sharing and coordination.
A tale of two organigrams: NICE and WHO
In seeking a benchmark organization that delivers a key public good, we looked to one shining star in the world of science and health with practical policy and programmatic applications: the United Kingdom’s National Institute for Health and Care Excellence, or NICE. Rather than organize around disease or biomedical specializations, NICE is organized around the types of products and activities that it delivers, distributed across seven directorates:
- A Center for Guidelines that produces guidelines for clinical care, public health, and social care;
- A Center for Health Technology Evaluation that develops guidance on new and existing treatments including medicines, medical technologies, and surgical procedures;
- A Health and Social Care Directorate to drive implementation of the guidelines generated in the two Centers for Guidelines and Health Technology Evaluation; and
- A Science, Evidence, and Analytics Directorate addressing the latest use of science, evidence, and data on NICE’s activities; with
- The remaining four directorates as operational: information technology, finance, human resources, and communications.
Importantly, NICE is not organized around any specific biomedical classification or disease area. This organizational structure has advantages in terms of resource sharing, as well as standardization. Experts for specific diseases can share and learn from other disease areas—which, by the way, are for the same patient or beneficiary population—as well as share scientific methods and tools for understanding and navigating the complex and ever-evolving landscape of knowledge. Grouping by activity minimizes the “my disease is the most important” type of “sibling rivalry” or “resource rivalry” when organized by biomedical siloes—rampant throughout global health.
NICE is far from a unique case. European countries have long operated HTA agencies, and other countries around the world—at all income levels—are beginning to use and institutionalize these tools, with support from the International Decision Support Initiative (iDSI), Health Technology Assessment International (HTAi), Bergen Centre for Ethics and Priority Setting (BCEPS), Africa Centre for Disease Control and Prevention (AfCDC), and others.
WHO’s opportunity for growing its cross-cutting role in clinical trial platforms
Cross-cutting functions of science, beginning from registering clinical trials, aggregating scientific databases, evidence synthesis, and policy recommendations, are a continuum of the practice of science that cut across disease areas. WHO has several opportunities to lead in these cross-cutting functions to enhance global health as well as pandemic preparedness.
The first area of such a cross-cutting function is the registration of clinical trials, through WHO’s clinical trials platform. Reporting clinical trials is crucial for the validity of science, due to the problem of publication bias, or the underreporting of null or ineffective studies (see the work by alltrials, for example). The inclusion of such studies about the lack of efficacy are as important as looking at studies which show efficacy.
But WHO’s role in this cross-cutting function should not end here. WHO has an opportunity to further lead in the building of agile clinical trial network platforms and infrastructure in ways that will be key for emergency and pandemic preparedness. Such preparedness of clinical trial infrastructure goes beyond policy discussion on ethical considerations. WHO needs to coordinate with Europe, US, and others further building such infrastructure. The G20 High-Level Independent Panel report on pandemic financing (p 41) also reinforced the need to address agile supply of medical countermeasures, which begins with contract design and incentives for R&D and ends in manufacturing and distribution.
WHO’s chance to expand scientific knowledge management
The second area of a cross-cutting function is the management of scientific databases of health research and studies, which aggregates scientific publications and literature. Managing new science is challenging because of the many sources, not only journals but increasingly new forms of publication, and requires interdisciplinary expertise in library sciences.
One key achievement of the WHO during the pandemic was the creation of the WHO COVID-19 Research Database. This database aggregates more than 700,000 research articles published across several databases including MEDLINE, PubMed, EuropePMC, and so on—but only on COVID-19 studies. WHO should be given kudos for developing such a database during a time of great crisis and need.
Moving forward, WHO has an opportunity to expand this function not only to COVID-19 but to non-COVID diseases as well. This “librarian” function of health knowledge and research should be streamlined across the WHO’s different boxes and siloes in ways that allows individual disease areas to tap into similar shared cross-cutting science library and knowledge resources. Today’s libraries live on the internet, and the management of information and science requires greater expertise in information technology, computer science, health informatics, and data science. In an era with tremendous misinformation and misuse of science, WHO leadership has a chance to shape how science-based institutions collect and aggregate knowledge in ways that lend to greater public trust in science.
Using evidence synthesis for informing policy recommendations
Knowledge from clinical trials or compiled scientific literature is inadequate on its own to make policy recommendations or guidance, let alone international or national decisions. Making poor recommendations or recommendations with opaque evidence synthesis can be at best irrelevant or at worst counterproductive, wasteful, or even harmful.
Throughout the pandemic, we saw the use and misuse of scientific trials and research articles in communicating biased positions or recommendations, which resulted in even greater mistrust of public health and science more generally. Making recommendations based on science should not be based on the whim of any one scientist or person but should require stakeholder engagement and institutional processes.
Evidence synthesis is the tool by which knowledge from different studies for a given intervention or risk is assessed for the quality of the study. Overarching recommendations are based on a rigorous and systematic approach to evidence synthesis. One crucial methodology that uses evidence synthesis is that of HTA—the key methodology used by UK’s NICE and other HTA agencies around the world.
HTA is an essential methodology that goes beyond reviewing and assessing the scientific evidence (or evidence synthesis). It goes a step further to draw not only on the efficacy and effectiveness, but also on the costs and the tools of systematic reviews, cost-effectiveness analysis, and stakeholder engagement in order to make a science-based recommendation (see Figure 1).
WHO has an opportunity to standardize HTA by streamlining organizationally, to follow through its resolutions related to HTA including a 2014 WHO resolution 67.23. WHO currently has HTA used by two distinct boxes and siloes in its organigram—one in a Health Systems, Governance, and Financing box and another in a Medical Devices and Diagnostics box. HTA cuts across many diseases and health conditions throughout the WHO organigram. As WHO identifies its common functions that cut across disease areas, WHO should develop a process for integrating HTA across disease areas.
Moreover, although WHO has a guidelines review committee and process for the development of guidelines which uses evidence synthesis, WHO’s use of HTA remains limited. Further, standardizing processes and methodologies for stakeholder engagement can help to improve the quality of recommendations—and prevent poor science communication and improve the trust in science. The ways in which evidence synthesis are conducted by stakeholder groups convened by WHO may well vary. For example, WHO has various advisory groups to engage scientists and experts into making recommendations, such as the SAGE, but what about for other disease areas? The ways to incorporate stakeholders including scientists, as well as lived experiences of patients and other vulnerable voices, should not be confined to any one disease area. Stakeholder engagement is thus also a cross-cutting function that is not confined to a single disease area—and used not only for guidelines but also in making recommendations.
Figure 1. Overview of the Health Technology Assessment Process
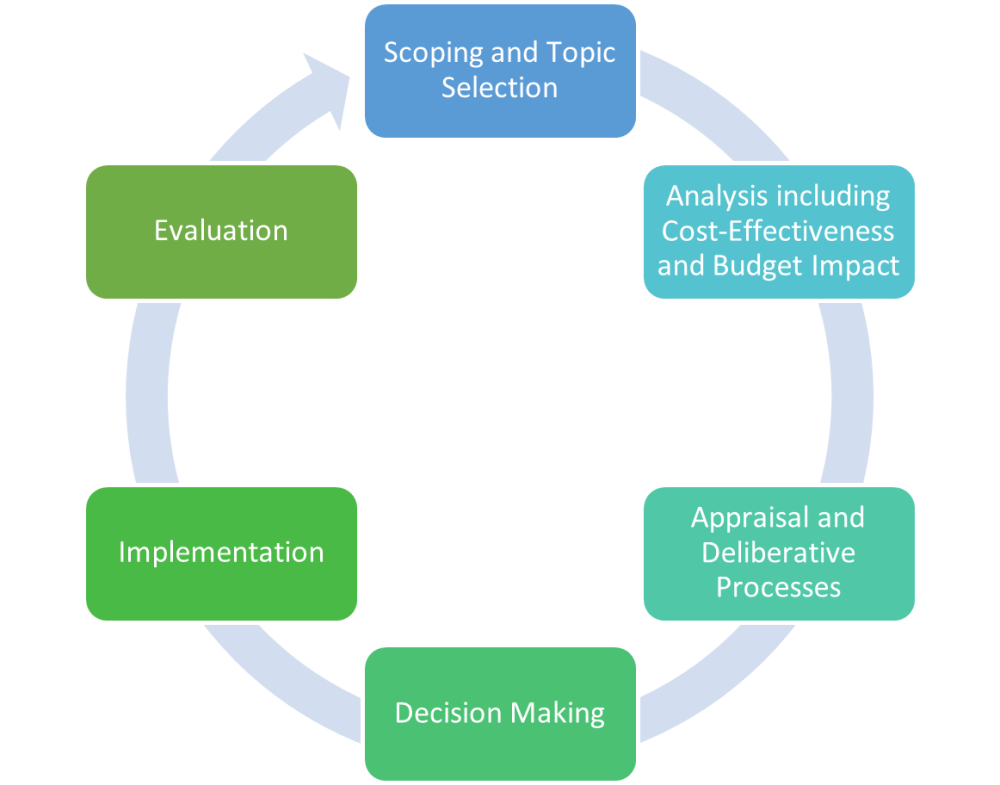
Source: Fan
Institutionalize and streamline global and local HTA functions in the WHO
This year marks the 30th anniversary of the 1993 World Development Report (WDR), which pioneered the use of evidence synthesis and cost-effectiveness in identifying a highly cost-effective package of interventions. The 1993 WDR was also instrumental in inspiring Bill Gates to invest in global health, because saving lives could be so cheap and cost-effective. Since then, the 1993 WDR has gone through two successive editions of the Disease Control Priorities: DCP2 (the 2006 second edition) as well as DCP3 (the third edition which comprised of nine volumes).
CGD, too, has long championed the use of HTA and priority setting in global health as forms of translating evidence to policy (see here, here, here, and here). CGD’s work in priority setting led to the incubation of the International Decision Support Initiative (iDSI), a global HTA facility that provides technical assistance to countries to institutionalize priority setting (although iDSI is closing at the end of 2023). iDSI has supported many countries to build local priority-setting institutions in order to generate local evidence about what works and at what cost.
The global health community has arguably lost sight of using HTA to inform scientific recommendations. The World Bank has no dedicated staff members working on the Disease Control Priorities or HTA more generally. The WHO does not consistently conduct HTA—even as other parts of the WHO continues to make global recommendations based on efficacy and effectiveness such as for masks.
The key point is for WHO to streamline its cross-cutting HTA standards and functions. This recommendation to streamline HTA across the disease areas in the WHO is also consistent with past recommendations for the WHO to have a chief economist (see here and here) who could work as part of the WHO chief scientist’s team.
Throughout the pandemic, WHO has been making science-based recommendations, guidance, and standards, based on a variety of expert groups amidst ever-evolving science. To up its game, the WHO needs to systematize the way it uses science across disease areas. The practice of science should lead to rigorous and trusted recommendations, guidance, or guidelines, which ultimately require evidence synthesis and HTA. To deliver on this core WHO service in ways that builds public trust, the WHO should work to reorganize, streamline, and institutionalize these cross-cutting functions.
With thanks to Sara Viglione and Prashant Yadav for helpful comments.
Topics
DISCLAIMER & PERMISSIONS
CGD's publications reflect the views of the authors, drawing on prior research and experience in their areas of expertise. CGD is a nonpartisan, independent organization and does not take institutional positions. You may use and disseminate CGD's publications under these conditions.
Thumbnail image by: Adobe Stock



