Recommended

Event
A Sustainable and Ethical Future for Health Worker Mobility
HYBRID
May 20, 2026 12:30—2:00 PM ET | 5:30—7:00 PM BST | 6:30—8:00 PM CEST
At the 79th World Health Assembly, Member States adopted landmark amendments to the World Health Organization’s (WHO) Global Code of Practice on the International Recruitment of Health Personnel. But what were these changes, and how can they be operationalised in practice?
Understanding the WHO Global Code of Practice
In 2004, recognising the impact of international health worker mobility on countries of origin, the World Health Assembly (WHA) mandated that its Director-General develop a non-binding code of practice. It was discussed at the first ever Global Forum on Human Resources for Health in 2007, baked into the resultant Kampala Declaration, and finally adopted by the 69th WHA in May 2010.
Crucially, the WHO Code discourages the “active recruitment of health personnel from developing countries facing critical shortages of health workers.” In a 2021 paper, we outlined how such “critical shortages” were defined. Currently, 55 countries (largely all in Africa) fall under this definition, from which “active recruitment” is discouraged.
However, the WHO Code has long been misinterpreted as banning all recruitment from these 55 countries. Yet recruitment is allowed as long as it is done within a government-to-government agreement that requires the country of destination to provide technical and financial assistance, aimed at strengthening health systems and health workforces.
Despite this, many destination countries are worried about engaging with countries with “critical shortages,” leading to painful situations. In Ghana, for example, trained nurses remain underemployed at home, and yet effectively “blocked” from migrating to destination countries in need of their skills.
Implementation of the WHO Code has been uneven
Yet the WHO Code and related frameworks remain voluntary international law, and implementation has been uneven. As has been documented by the WHO, and as we are exploring in current research with the World Bank, most government-to-government agreements are:
“explicitly aimed at addressing health worker shortages in health systems of destination countries. It is often unclear in these agreements, however, how health service delivery in countries of origin will be maintained, and or what the expected benefits migration can generate for the country of origin’s health system…”
Destination countries can, by and large, attract the health workers they need without having to provide concurrent investments. So why should they? As we recently documented alongside the UK’s All Party Parliamentary Group on Global Health & Security and the NGO Global Health Partnerships, destination countries benefit substantially—both financially and securing needed skills—from international recruitment. This provides a strong ethical and moral case as to why they should invest.
Yet origin countries, for the most part, are not yet demanding the investments that they need and rightly deserve. Many are signing government-to-government agreements which contain vague language about proportionate co-investment, and do not include any robust monitoring and evaluation frameworks to track such investments. This is slowly shifting, but such countries need much more support in defining their investment plans and advocating for their rights in these negotiations.

Speakers from the CGD WHA side event, “A Sustainable and Ethical Future for Health Worker Mobility”
These were the subjects covered by our WHA side event, held two days before the WHO Code amendments were due to be discussed. Speakers from the World Bank, OECD, International Organization for Migration, WHO, Global Health Partnerships, and the governments of Kenya and the Philippines, outlined why a new system is needed: one that prioritizes meaningful cooperation, takes a whole-of-government approach, and turns health worker mobility into a tool for economic development and health systems strengthening.
The amendments are a step in the right direction, but enforcement will be challenging
We were therefore delighted to see that the newly adopted amendments strongly encourage destination countries to partner with origin countries on “mutually beneficial strategies and targeted co-investments in specific areas of the health workforce and health systems.” Language around “proportional benefits” and “skills partnerships” even made it into the resolution text, signalling the impact CGD and its many partners are having in this space.
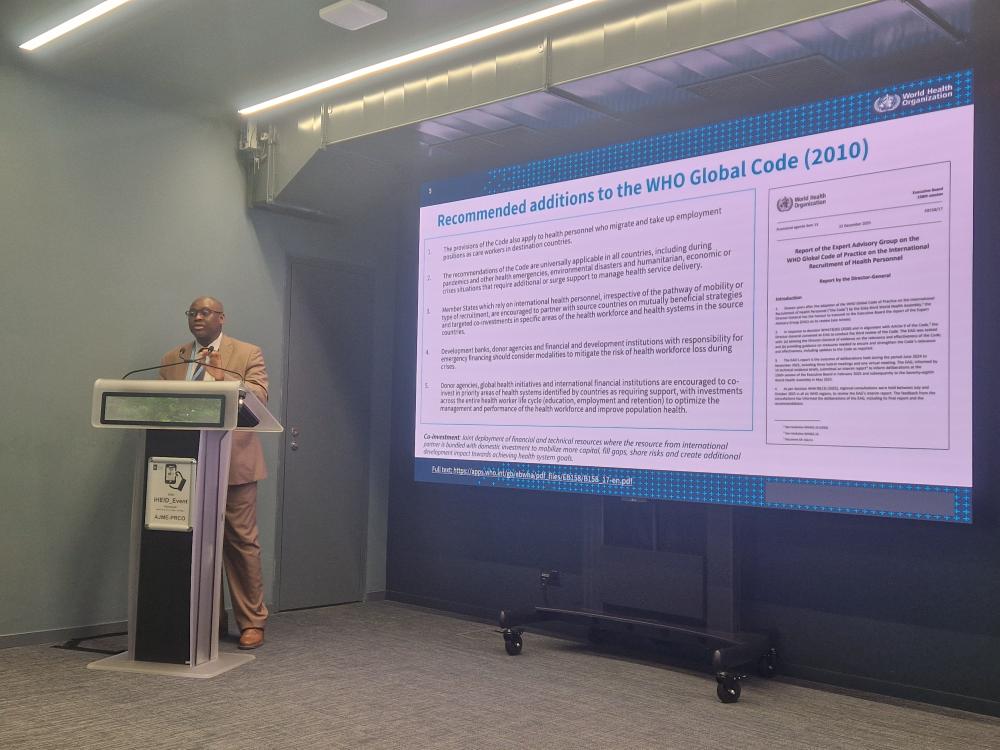
Khassoum Diallo, Unit Head, Health Workforce at the WHO presenting the amendments at CGD’s event
Implementing and enforcing this will be more difficult, particularly in an era when the WHO is suffering from a reduced headcount and budget. We agree with the comments made by Jim Campbell in our event: take a selection of the willing top 10 origin and destination countries, and bring them together in an informal setting to discuss what a meaningful partnership and investment model looks like. We facilitated similar conversations in March, and hope to continue these to agree on practical solutions in the future.
The amendments to the WHO Code also included two other interesting provisions. Firstly, it will now apply to care workers, something we at CGD have long sought to clarify. Yet, as Jean-Christophe Dumont from the OECD mentioned, “this is not the same game.” By 2030, there will be about 84 million health workers and 475 million care workers. This is a sector with high levels of exploitative recruitment; large numbers of unpaid, unemployed, and under-employed workers; and a lack of meaningful investments in formal skills training, certification, and regulation. How to operationalise the WHO Code for the care sector is a huge question and challenge that we hope to tackle.
Secondly, an amendment confirmed that the WHO Code applies during pandemics and other emergencies which require additional or surge support: an inclusion relevant in the aftermath of COVID, which emphasised the management gaps of health workers between origin and destination countries. Moving towards a world where we have a globally mobile cadre of health workers who can be deployed at a moment's notice to contain disease outbreaks is certainly a worthwhile goal. But, again, it is unclear how the WHO Code could be implemented and enforced in such pressing and chaotic times. How would such agreements be negotiated? Would they merely support short-term or temporary mobility? What would the “proportionate” investments look like? And who really holds the power in such situations?
More questions than answers
We applaud the work of the Expert Advisory Group, the WHO, and all those who had a hand in developing these amendments and getting them over the line. There are some very welcome clarifications in the text, and it is heartening to see a stronger commitment to co-investment. Of course, it remains to be seen how these new amendments can be implemented in practice, and how these efforts can be integrated into health system strengthening more broadly.
We plan to work with the World Bank and our broader partners on these issues in the coming years, so please do get in touch to discuss!
Topics
DISCLAIMER & PERMISSIONS
CGD's publications reflect the views of the authors, drawing on prior research and experience in their areas of expertise. CGD is a nonpartisan, independent organization and does not take institutional positions. You may use and disseminate CGD's publications under these conditions.



