Recommended
Blog Post
Six Lessons from 10 Years of iDSI

This blog summarizes an article published as part of a special issue of Health Systems & Reform, ‘Building Institutions for Priority Setting in Health.’ Access the special issue online here.
Colombia embarked on a major health sector reform in 1993, introducing a mandatory universal social health insurance system and a priority-setting system featuring a health benefits package (HBP). This HBP defined which interventions were covered by the system, whom it was for, and at what costs. In the thirty years following the reform, Colombia has made impressive strides towards universal health coverage (UHC), financial risk protection, and ensuring equitable access regardless of ability to pay. However, despite recent accomplishments and significant health care budget increases, the Colombian health system has faced substantial challenges, and its budget has fallen short of meeting growing demands.
In a new article for a special issue of Health Systems & Reform, we delve into the evolution of priority setting and HBPs in Colombia since the pivotal 1993 health sector reform. We examine the key historical milestones, explore influencing factors, and weigh the pros and cons of various approaches employed over the past thirty years. Our discussion draws out lessons learned, ongoing challenges, and future perspectives.
How HBPs have evolved in Colombia over the past thirty years
The evolution of HBPs in Colombia over the past thirty years can be divided into two phases of major reform. Phase 1, spanning from 1993 to 2017, focused mainly on inclusions due to an explicit priority-setting process via a positive list, or HBP. The second phase, starting in 2017, abandons the HBP approach with a positive list and moves to an implicit approach that covers, in theory, everything for everyone, excluding a narrow negative list of services and health technologies. Both approaches were implemented with different institutional and governance arrangements, criteria for inclusion or exclusion, and stakeholder participation.
Phase I: An Explicit Priority-Setting Process for Inclusions, 1993-2017
Throughout the first phase, the explicit priority-setting process and the institutional arrangements to make coverage decisions in the Colombian health system became more stable and transparent. As institutions were created and terminated, the process and responsibilities became clearer and more robust. Specifically, more steps and increased specialization were achieved, along with broader stakeholder engagement.
The first phase can be split into three distinct stages to understand the evolution of the priority-setting process.
Figure 1. Health technologies assessment process and key actors before the statutory health law, from 1993-2017
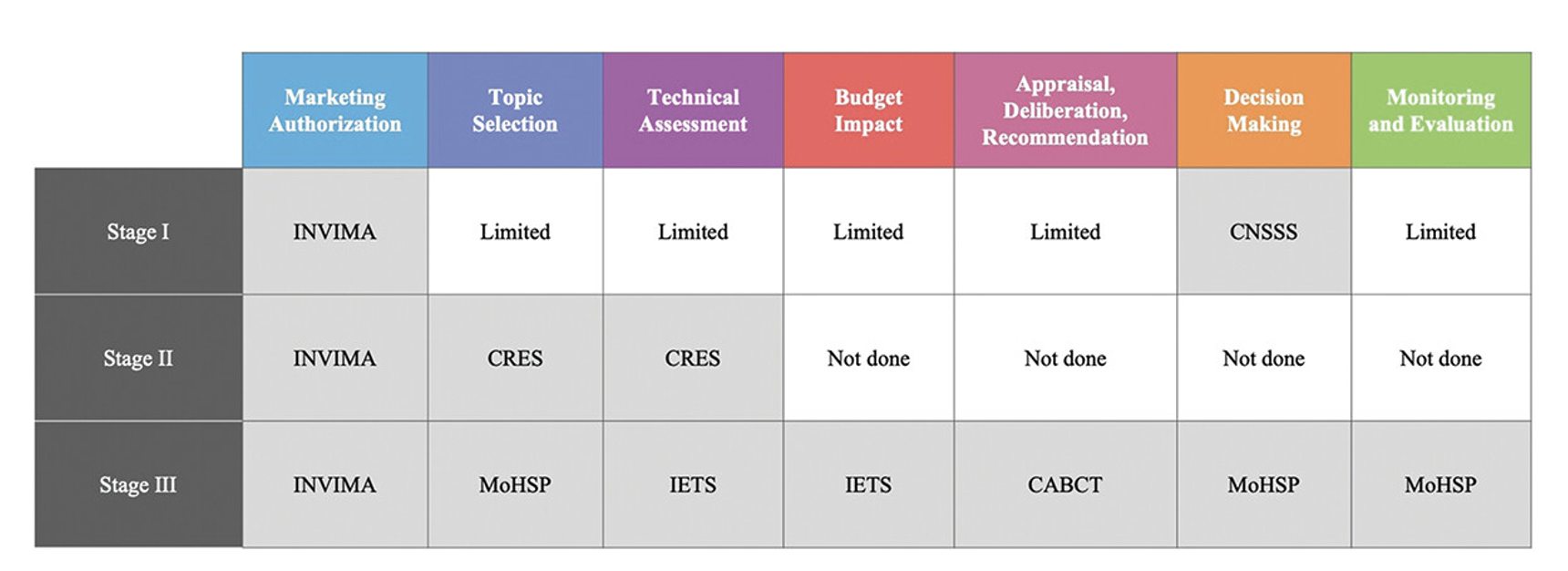
Source: https://www.tandfonline.com/doi/full/10.1080/23288604.2024.2343174
Phase II: A new exclusion process, 2017-present
The second phase kicked off in 2017 with the enactment of the statutory law of 2015, which ratified the right to health as an autonomous fundamental human right in Colombia. This law catalyzed a new exclusion process, mandating the Colombian government to move from marginally expanding the HBP with inclusions to assuming that all health services and interventions were covered, except those meeting specific circumstances. The Ministry of Health and Social Protection (MoHSP) implemented a new process for exclusions that incorporated consultations with groups potentially affected by any inclusion, and important participatory and transparency features. By June 2023, a small minority of less than 1 percent of technologies approved by the regulatory agency had been included in the list of exclusions.
Advantages and disadvantages of each period of reform
Each period of reform has its own advantages and disadvantages, offering valuable lessons for other low- and middle-income countries (LMICs) as they face pressure to shift to negative lists that define the basic health package by what’s excluded rather than included.
Under the inclusion-based priority-setting system, HBPs played a crucial role in expanding coverage and working toward UHC in Colombia. They established explicit, legal entitlements for Colombians by determining which services would be available and to whom. HBPs also helped calculate premiums paid to insurers, and signal priority services to clinicians and patients. However, limitations set by the HBP may have made clinicians feel constrained, and patients could have perceived that key technologies were not included without further explanation. Further, insurers may have used the HBP to deny care. Social pressures including Colombians embracing the right to health ultimately prompted the shift from the inclusion-based priority-setting system to an open approach with minimal exclusions in 2017.
This change raised several concerns. First, issues of transparency, legitimacy, and financial sustainability. Patients and providers may presume that all services are covered, but the reality is, neither health care expenditure nor the premium paid to insurers have increased to accommodate all the theoretically covered services. Second, delays in exclusion as new technologies and medications come to market may expose insurers to an increased early demand for high-cost technologies. This might turn into implicit rationing with the risk of favoring new, high-cost technologies in urban areas which might lead to increased inequity. Third, because cost effectiveness cannot be used as an exclusion criteria, some technologies and medications may not give the biggest bang for the buck. However, shifting to a negative list also had several benefits. It provided clarity to stakeholders that insurers cannot deny health services just because they were not listed in the HBP, and promoted medical autonomy by reducing bureaucratic and administrative barriers. Additionally, by receiving funding ahead of time based on estimates rather than seeking reimbursement after treatments were paid out, insurers can better manage clinical and financial risk.
In sum, shifting from a positive to a negative list brought about a tension between two views: a view embracing health as a fundamental right, and when taken to the extreme, pushing for guaranteed health care regardless of financial considerations; and a second view which argues that available funding must determine what is covered and that value for money should be maximized for any budget. While processes and methodologies have become more transparent and stable over the past thirty years, limitations still exist as the concept of opportunity cost is not adequately embedded into decision-making.
Policy options for the Colombian government
In this moment of reform, we offer six policy options for the Colombian government to consider as they reflect on how to determine priorities within financial means, while also guaranteeing a system that delivers on the promise of health as a fundamental right.
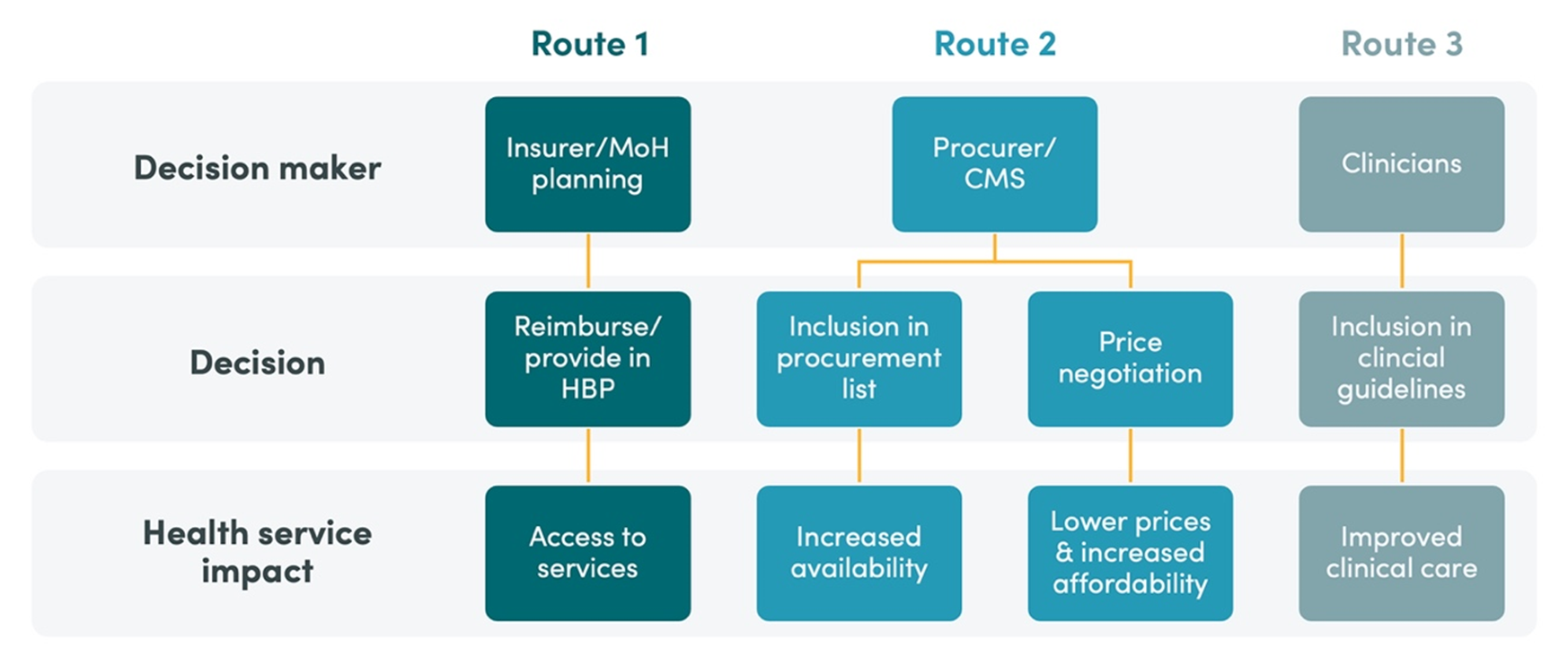
1. Strengthening priority-setting at lower levels within the health system: Insurers and health care providers could conduct their own evaluations and decisions regarding covered benefits and associated costs, which could increase health care quality and potentially lead to quicker responses, localized strategy, and an increased reach and impact.
2. Alternative processes to deal with health technologies with low cost-effectiveness: While the MoHSP cannot use economic evaluation to exclude products based on cost-effectiveness, these methodologies could be applied for other purposes, such as price regulations, negotiations and the development of standard treatment guidelines. Our article proposes a few techniques that the MoHSP could use to prevent high-cost products from entering the Colombian market without adequate stewardship.
3. Deploying alternative options for funding insurers: Adequate incentives should be implemented, including changing how the premium is calculated and better ex-ante and ex-post adjustments, to steer insurers to better manage clinical and financial risk and deliver high-value quality care.
4. Increasing efficiency in the system: Tackling inefficiencies in the form of excess costs in producing a given output would help the system achieve more health for the money. Options include demand aggregation and centralized procurement of expensive technologies, increased use of generic and biosimilar medicines, and tackling waste, corruption, and fraud.
5. Improving monitoring and evaluation: The MoHSP could systematically and routinely measure the services provided and the quality of such services to measure effective coverage and identify and address implicit rationing or signal inadequate consumption patterns.
6. Strengthening stakeholder participation: It is crucial to increase effective engagement of stakeholders in fundamental discussions such as the financial sustainability of the system, the importance of maximizing health benefits, of following priority setting, and the need to incorporate new technologies at fair prices.
Colombia’s evolution of priority-setting over the past thirty years offers several lessons for other low- and middle-income countries interested in institutionalizing evidence-based priority-setting. Learning from its successes and failures is key to informing current and future discussions on how to pursue universal health coverage.
Topics
DISCLAIMER & PERMISSIONS
CGD's publications reflect the views of the authors, drawing on prior research and experience in their areas of expertise. CGD is a nonpartisan, independent organization and does not take institutional positions. You may use and disseminate CGD's publications under these conditions.



