Recommended

CGD NOTE
COVID-19 and Oxygen Supply
The COVID-19 pandemic is a critical illness crisis, with more than two million deaths worldwide and hospitals overburdened with 67 percent of COVID-19 admissions requiring oxygen. With the emergence of new variants and the rise of second or third epidemic waves, there is unprecedented demand for oxygen as a life-sustaining, first-line therapeutic and an essential resource when caring for the critically ill.
However, countries around the world are reporting oxygen shortages on a daily basis, especially low-and-middle income countries (LMICs) such as Nigeria, Zimbabwe, South Africa, Pakistan, Brazil, India, and Mexico. Media reports also suggest black markets are emerging, and prices for medical oxygen have increased several fold in Peru, Mexico, Pakistan, and Brazil.
We examine some of the likely causes of oxygen shortages in LMICs and suggest policy solutions. These include improving dialogue between the multilateral development banks and countries on oxygen needs and demands; establishing national task forces; and building partnership between countries, the World Bank, and other ACT-Accelerator (ACT-A) agencies to improve financing, contracting, regulation, infrastructure, and clinical use of oxygen.
Why are there shortages of medical oxygen?
Many countries have been slow to prioritise medical oxygen, and the World Bank reports that very few countries (e.g., Zambia) have formally requested emergency response funding to procure medical oxygen. We posit some reasons that may be behind the low priority:
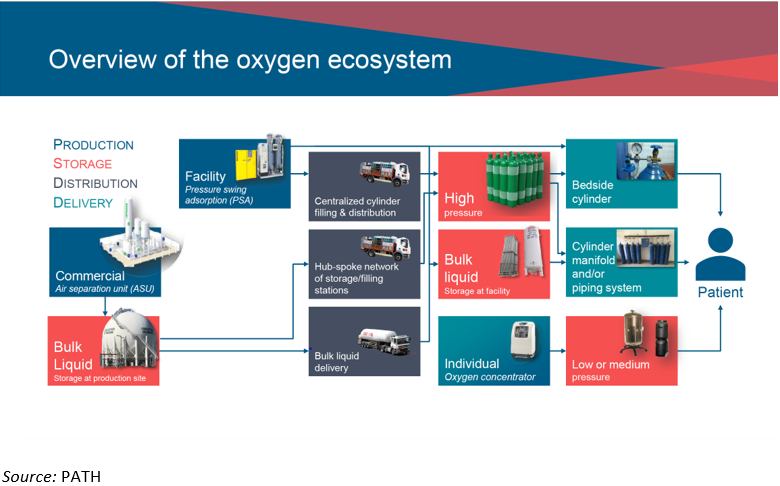
- Scale up of medical oxygen is a complex, specialized process involving many actors (see Figure 1) that may create barriers for new firms to enter the market and easily scale up supply.
- National and global responses have prioritised maintaining current services; developing test, track and trace systems; and developing and providing pharmaceutical therapeutics for COVID, to the detriment of essential critical care including oxygen.
- Many health systems decentralise oxygen procurement to individual hospitals, resulting in little forward-looking planning to invest in larger-scale and longer-term oxygen solutions (e.g., Indonesia).
- COVID-19 emergency financing facilities have been complex where countries have had to navigate simultaneous submissions for emergency response funding amongst multiple donors and financiers, which are logistically challenging and resource-intensive exercises during a crisis.
- The regulatory legal and governmental framework for oxygen and related medical equipment in many LMICs is still relatively nascent, and ensuring safety, identity, strength, quality, and purity can be challenging.
- Funding for oxygen was also more likely to be supported by World Bank loans, which may have been less attractive than grants or donations (e.g., tests via Africa CDC).
Figure 1. Overview of the complex oxygen ecosystem
Global responses to shortages in medical oxygen
In April 2020, the World Health Organization set up the ACT-Accelerator to expedite the development, production, and equitable access to COVID-19 tests, treatments, and vaccines, with the aim of speeding up the end of the pandemic. The ACT-Accelerator originally had three pillars focused on diagnostics, treatment/therapeutics, and vaccines. While medical oxygen has always been central to COVID-19 care, the therapeutics pillar has only focused on improving access to pharmaceutical treatments such as dexamethasone or colchicine. A fourth pillar which focuses on health system strengthening, including medical oxygen provision, was added in November 2020 in the second publication of ACT- Accelerator. This pillar, however, has been neglected, with only 5 percent of its budgeted needs actually funded by donors ($436m).
On the other hand, the World Bank has provided funding to LMICs with over $160 billion committed to the pandemic response. This includes $8 billion that was approved in March/April 2020 for COVID-19 country response. Whilst countries can apply for this funding to cover investment in oxygen supplies, as mentioned, its use has been rare so far. Other multilateral agencies such as the World Health Organization and UNICEF had some success at the start of the pandemic in making concentrators, pulse oximeters, and consumables available but this was not enough to satisfy the current medical oxygen needs.
A purchase receipt for oxygen cylinders is tagged onto an oxygen cylinder manifold system in Uttar Pradesh, India. Credit: PATH/Zach Clemence
Short-term recommendations
Given the large and immediate need for medical oxygen across LMICs to mitigate deaths due to COVID-19, here are some ideas on how to immediately prioritize medical oxygen as an essential component of the COVID-19 response:
Countries need national and formal task forces to prioritise medical oxygen. Countries should consider establishing formal task forces that can aid in strategically ensuring medical oxygen remains a priority and shows up in every country COVID-19 response project proposal. Countries can also ensure that more manufacturers are registered in-country and that planning focuses on identifying the right modes of delivery of oxygen to patients considering the infrastructure in place, enabling national procurement to be realized more efficiently during the crisis.
More international analysis and dialogue between the multilateral development banks and countries on oxygen needs and demands. This will pave the way for easing access to financing for medical oxygen in countries.
ACT-Accelerator partners should recognise and fund medical oxygen as an essential COVID-19 therapy and create regional frameworks for countries to engage different suppliers. The ACT-Accelerator Facilitation Council should recognise medical oxygen as an essential COVID-19 treatment, making funds more available and easier to access for deployment of medical oxygen related interventions. ACT-A should coordinate financing sources and collate requests to ensure a match between requests and financing. Additionally, ACT-Accelerator partners can play a strategic facilitation and advocacy role between country-specific decision-makers and regional and national medical oxygen suppliers. Such frameworks have already been implemented for other utilities and would allow for rapid, regulated, and strategic procurement and distribution.
Provision of technical assistance to strengthen health systems for maintaining and using medical oxygen. The complexity of oxygen scale-up, coupled with the other clinical needs of the critically ill recipients of oxygen therapy, necessitate systems thinking for sustainability and an optimised impact on the quality of patient care and improved outcomes of oxygen. Technical assistance, training of health workers, and improved processes for essential emergency and critical care, building capacity in equipment maintenance and biomedical engineering in facilities, and support to medical oxygen infrastructure development should be provided.
Medium-term recommendations
Some countries had already put strategies in place before the pandemic; for example, Ethiopia, Uganda, and Nigeria established roadmaps between 2015 and 2019 to scale up the supply and availability of medical oxygen in hospitals as part of their health sector agenda. However, in order to tackle the medical oxygen challenges faced by all LMICs, we discuss medium-term strategies that can aid in strengthening the market and sustainably promote adequate and equitable supply of medical oxygen at affordable prices for LMICs in the future.
Generate evidence to identify cost-effective national strategies for medical oxygen scale-up and use in different settings. Better evidence on the scale-up and optimal use of medical oxygen and care of critically ill patients in LMICs is needed. Such evidence can be generated by building on ongoing projects investigating the current state of care and costs and the cost- effectiveness of implementing essential emergency and critical care. Resources like PATH’s medical oxygen delivery toolkit and the creation of suitable indicators for monitoring and evaluation can also play a role in generating better evidence.
Develop and optimise multipronged, context-specific medical oxygen supply chains and infrastructure. Governments, with global stakeholder support where needed, should develop national oxygen strategies and establish a diverse mix of public and private sources with different oxygen supply options that solves their context-specific challenges. For example, Kenya used a multipronged approach which included public funding (plants at public hospitals), public-private partnerships (e.g., Hewatele partnership), and private companies (e.g., BOC Kenya) to set up local medical oxygen plants across the country. This has increased the availability of medical oxygen in Kenya, leading to a drop in the price of about 50 percent.
Develop biomedical engineering capacity among public and private sector service providers. Scaling up medical oxygen infrastructure must be coupled with improving local biomedical engineering capacity in LMICs. Such capacity-building exercises can ensure that existing medical oxygen plants and equipment are well maintained, and new infrastructure can be designed locally and sustainably. In addition, improving capacity will foster innovation, modification, and construction of new equipment that suits the local setting. For example, solar-powered medical oxygen concentrators have been developed and are currently being piloted in Haiti and Uganda to address the problem of intermittent electricity supply in rural areas.
Improve local capacity for health workers in essential emergency and critical care to increase the use of medical oxygen and patient survival. Essential emergency and critical care consists of effective life-saving actions, of low cost and complexity, and is appropriate for all hospital settings. Local health workers and technicians should be trained in the provision of essential emergency and critical care, which includes implementation of effective delivery of medical oxygen and other life-saving care to reduce the number of deaths due to COVID-19. This focus would leave health systems strengthened to reduce preventable deaths beyond the pandemic.
Encourage a stable business environment for countries and suppliers to engage and do sustainable business. Global partners should work with countries and medical oxygen suppliers to ensure that a national oxygen strategy (medical oxygen technology, country needs, laws, standards and regulations) is implemented favourably to conduct ethical and sustainable oxygen-related businesses. Interventions like bulk purchasing through regional agreements or the signing of long-term contracts can help to ensure that a reliable medical oxygen supply reaches those who need it most.
Conclusion
Any response to improving oxygen supply is too late for the thousands who have died due to COVID-19 so far. But given the simple recommendations we have shared, if there was ever a time for global and national actors to increase the prioritisation of medical oxygen and improve essential critical care, that time is now.
We thank Leith Greenslade for her valuable insights for this blog.
Topics
DISCLAIMER & PERMISSIONS
CGD's publications reflect the views of the authors, drawing on prior research and experience in their areas of expertise. CGD is a nonpartisan, independent organization and does not take institutional positions. You may use and disseminate CGD's publications under these conditions.
Thumbnail image by: PATH/Zach Clemence


