Recommended

Event
Best Buy Lists and Priority Setting Tools for Universal Health Coverage
VIRTUAL
August 29, 2023 10:00—11:00 AM ET / 3:00-4:00 PM BST
There are few health conditions that impact as many people as visual impairment. Some 1.1 billion people, the vast majority in low- and middle-income countries (LMICs), live with uncorrected refractive error, cataracts, and other eye diseases. A recent study commissioned by the Seva Foundation is the first to systematically examine the evidence supporting the benefits of eyecare beyond health, and conduct return on investment (ROI) calculations. The researchers found a $36 to $1 ROI from providing glasses or cataract surgery, comparable to some of the best uses of resources in the development sector. Overall, there is a compelling case that policy makers should pay more attention to visual impairment: an enormous yet tractable problem with potentially highly cost-effective solutions.
Visual impairment is a neglected health problem
Recently, the World Health Organization (WHO) launched SPECS 2030—an initiative to increase the coverage of refractive error services. It signals an increasing awareness of a large and historically under-appreciated global health challenge. Around the world, 1.1 billion people suffer from visual impairment—more than the number of people affected in a given year by HIV/AIDS, malaria, tuberculosis, cancer, and heart disease combined. Yet eye care is under-acknowledged, not mentioned at all in the Sustainable Development Goals, and it is underfunded, receiving 0.06 percent of official development assistance and minimal public funding in LMICs.
Despite neglect on this topic, eyeglasses—the primary ‘technology’ to address visual impairment—are inexpensive and well established (there are few development interventions we know of that have a 700-year-old track record!). The cost of eyeglasses is around $5 per frame. Coupled with reasonable estimates for distribution, screening, and diagnosis costs, providing one person with clear vision requires ~$10 per year in LMICs. Cataract surgery, which can be delivered safely and effectively for a few hundred dollars in LMICs, leads to longer lasting benefits and has a similar average annual cost.
Huge returns of 36:1 in addressing visual impairment
The recent study, commissioned by the Seva Foundation and published in the Bulletin of WHO, is the first to systematically examine the evidence supporting the benefits of eyecare beyond health (note: one of us is the lead author on the study). Specifically, the systematic review looked for studies published in the last 20 years that documented productivity improvements at work, learning gains in school, or income benefits within households due to providing glasses or cataract surgery. The comprehensive search revealed 21 case studies across 10 LMICs, documenting benefits as large as a 67 percent increase in farmer profit from correcting myopia in Cambodia to halving poverty in vulnerable Indian households after cataract surgery. Using evidence on the costs of delivering glasses or cataract surgery, the study assesses the economic return on investment (ROI) in each case.
Their finding was remarkable: $36 to $1 ROI at the median (Figure 1). This figure is comparable to some of the best uses of resources in development sector, as recently identified by the Copenhagen Consensus Center, such as nutrition interventions, agricultural research and development, and insecticide-treated bed nets.
Figure 1: Returns from the provision of glasses and cataract surgery in LMICs
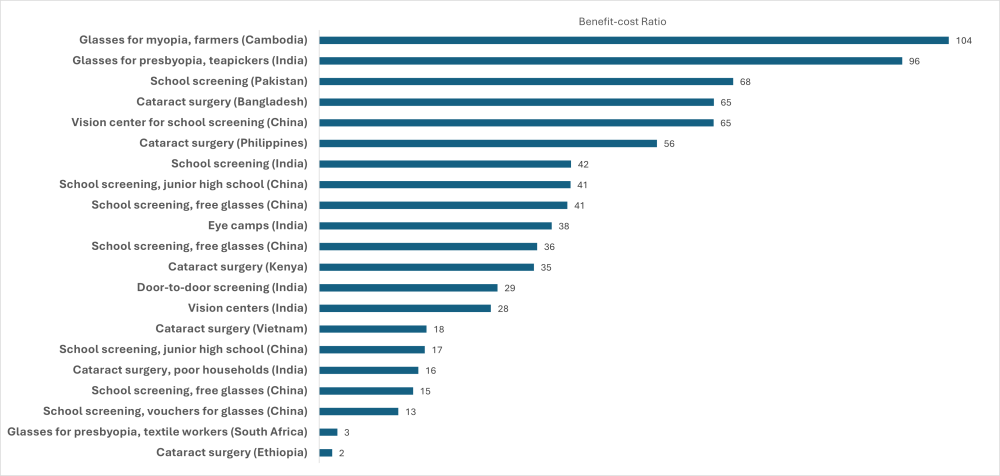
Source: Adapted from Wong, Brad, Kuldeep Singh, Bryce Everett, Kieran S O’Brien, Thulasiraj Ravilla, Rohit C Khanna, Heidi Chase, and Kevin D Frick. 2023. “The Case for Investment in Eye Health: Systematic Review and Economic Modelling Analysis.” Bulletin of the World Health Organization 101 (12): 786–99. https://doi.org/10.2471/BLT.23.289863.
A quick summary of a few case studies best illustrates these remarkable returns. In Assam, India, a randomized-controlled trial revealed that providing eyeglasses to workers resulted in a 22 percent increase in daily tea-picking productivity. Translating to thousands of dollars of extra agricultural output over multiple harvest seasons, the benefit far exceeded the one-off $20 cost of diagnosing and providing glasses. In another case study, the provision of glasses to school children in China, where half of children and adolescents are myopic, provided learning equivalent to half a year of business-as-usual schooling for a $15 pair of glasses. In Kenya, providing cataract surgery increased household expenditure by $360 per year (36 percent) for a one-off cost of $70. This last finding is especially notable because the surgery was provided to older members of the household, who were less likely to work. This suggests that eyecare may have indirect effects on household income generation, likely by alleviating substantial caregiver burdens.
The systematic review also highlighted some important limitations of the evidence. First, not all of the studies had robust methods, with roughly half presenting a moderate or serious risk of bias. Second, the confidence intervals on the estimated returns were large. Third, there was no evidence from certain regions such as Latin America and Caribbean and from some high-prevalence countries like Indonesia. Remarkably, all high-quality studies of vision correction in students came from just one country: China. These limitations highlight the need for more high-quality research across different contexts to validate the high returns from vision correction (or otherwise).
As an interesting postscript, several months after the systematic review was published, the results of an eyeglasses randomized-controlled-trial (RCT) in Bangladesh were revealed. The RCT showed that individuals provided with glasses for near-vision impairment experienced 33 percent higher incomes at endline, jumping from $35.30 to $47.10 per month. As a back-of-the-envelope exercise (and noting that glasses are usually replaced every three years), this suggests that eyeglasses might boost individual incomes in this context by $425. Assuming a cost of diagnosis and glasses of $10–$30, the benefit per $1 of cost is $14–$42—a large return and well within the range suggested by the systematic review.
The political economy of eyecare
With such a large problem that can be solved at relatively low cost, why has eyecare failed to capture the attention of development professionals and policy makers? Part of the reason could be that there are limited health gains from vision correction. The disability weight for refractive error implies a health loss equivalent to only 0.3 percent to 1.1 percent of a healthy life year. Battling an array of health challenges such as infectious disease, child mortality, and undernutrition, it is easy for health ministries (and their funders) to deprioritize vision correction. Yet anyone with glasses (including both of us!) intuitively understands that clear vision has implications that go well beyond the health benefits. Being able to see clearly is critical for living a productive and fulfilling life. The new study published by WHO clearly articulates the broad benefits extending far beyond health.
Similarly, other sectors that could benefit greatly from the provision of eyecare, such as education, manufacturing and agriculture might not be aware that vision correction could be a cost-effective intervention to help meet their goals of learning and productivity. Even if they were aware of its benefits, they would not have the capability to implement vision screening. Therefore, expanding eyecare is likely to require cross-sectoral collaboration between health and non-health sectors. Forthcoming work from the Disease Control Priorities project may help to conduct broader, comparable cost-benefit analyses of non-health interventions, but this new study highlights the value of conducting broader economic analyses for interventions in the health sector.
Encouragingly, the systematic review demonstrated that in most cases the benefits to vision correction were financial such as increased income or higher productivity. Individuals and businesses could partially fund some of the estimated $24.8 billion needed to eliminate preventable vision impairment. Indeed, many eyecare providers in LMICs, such as the pioneering Aravind Eye Care System in south India, operate a social-private model where those who can pay cross-subsidize those who cannot.
Overall, there is a compelling case that policy makers should pay more attention to visual impairment: an enormous yet tractable problem with potentially highly cost-effective solutions.
Topics
DISCLAIMER & PERMISSIONS
CGD's publications reflect the views of the authors, drawing on prior research and experience in their areas of expertise. CGD is a nonpartisan, independent organization and does not take institutional positions. You may use and disseminate CGD's publications under these conditions.
Thumbnail image by: Louisa Kiggwe/ Flickr



