UNAIDS recently convened a diverse group of experts to discuss how UNAIDS should go about estimating the post-2015 cost of the HIV/AIDS response. Participants opinions varied on most topics: whether estimates should assess the cost of treating all HIV infected people as soon as they are infected (the “Universal Test and Treat” option) or that of a less ambitious treatment policy; whether spending on poverty reduction and gender empowerment should be included in the cost estimates and, if so, on how to cost these “critical enablers.” But on one question, there appeared to be virtually unanimous agreement: donors and countries should increase the frequency, the granularity and the precision of HIV infection surveys.
There are two complementary approaches to measuring the “population prevalence” of a disease (i.e. the proportion of the population infected on a given date): population based surveys and sentinel surveillance of defined populations at higher risk. In the 1980’s population surveys were attempted in a few countries, including Uganda, Rwanda and Mexico, but they were costly and sometimes missed people in key population groups, such as prostitutes, injecting drug users or men who have sex with men. In response to these challenges, UNAIDS recommended that countries rely primarily on smaller, special purpose surveys of easily reached populations (e.g. women visiting antenatal clinics or prostitutes who frequent specific truck stops.) Although epidemiologists recognized these surveys might over-estimate the infection rate of the general population, they believed that the trends within these so-called “sentinel” groups would predict the trend in the overall population and that rules-of-thumb could be applied to arrive at a national estimate from the infection rates in these special groups.
However, in recent years epidemiologists have come to recognize that sentinel surveillance data on HIV, while essential, are insufficiently accurate and granular to understand the dynamics of an HIV epidemic in real time – and therefore insufficient to control the epidemic.
The evolving understanding of the complementarity between sentinel surveillance and population-based general surveys is well summarized by Peter Ghys, acting UNAIDS Director of Strategic Information and Evaluation. In the figure below, he demonstrates how a single population-based survey in 2007 enables statisticians to “correct” the trend line they had previously estimated from sentinel surveillance at antenatal clinics. Note that in addition to a substantial downward adjustment in the trend HIV prevalence in the country (from the blue trend line to the yellow one), the population-based survey also enabled the statisticians to improve the precision of their estimate for every past year (as represented by the thin region demarcated by dashed yellow lines compared to the fatter one between the dashed blue lines).
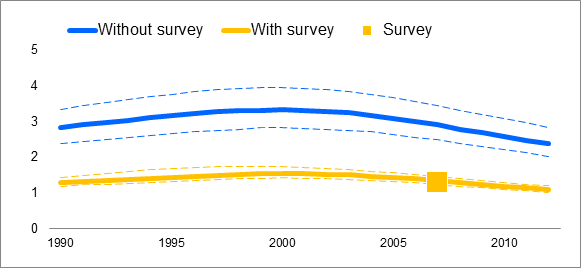
Source – Peter Ghys’ presentation at CROI, 2014.
More frequent and granular population-based HIV prevalence data would certainly be useful to technocrats who guide a national HIV program. But Tim Hallett and I have argued that better data has even more potential value, because it is the foundation on which an innovative donor could join forces with a national HIV prevention champion to design and implement a “cash-on-delivery” system of bonuses for effective HIV prevention.
How much would improved frequency and granularity of HIV prevalence surveys add to the future cost of HIV/AIDS programs? Peter Ghys estimates that a relatively simple HIV survey can cost 1.5-2.3 million dollars, while a more complex one can cost as much as 4-7.5 million dollars. The Kenya Aids Indicator Survey in 2012 was one of the more complex, but its cost only represented 1% of Kenya’s total annual investment in the AIDS response.
And other experts have weighed in on this topic. John Stover of the Futures Institute points out that, there are approximately thirty countries with generalized epidemic where conducting national surveys would be a practical option. If these surveys were conducted every two years, as recommended by CDC, they would cost approximately 90 million dollars per year. While this may seem expensive to some, Brian Williams of SACEMA suggests that compared to the approximately 20 billion dollars that are currently being spent on HIV in low and middle income countries, the cost of surveys represent only 0.4% of the total budget. Jeffrey Eaton of Imperial College London adds that instead of fielding a survey every two years, some countries might want to emulate Senegal’s continual rolling household survey, which would avoid startup costs, maintain a cadre of skilled professional surveyors and allow real time updating of HIV prevalence and incidence trends.
In the past few years, surveys have become an essential tool in informing national HIV and AIDS estimates and they have an important role to play in shaping policy. Now is the time to dramatically improve their frequency, granularity and precision as the foundation for improved program implementation. The first step is including this strengthened survey function in estimates of the cost of the future HIV/AIDs response.
Topics
DISCLAIMER & PERMISSIONS
CGD's publications reflect the views of the authors, drawing on prior research and experience in their areas of expertise. CGD is a nonpartisan, independent organization and does not take institutional positions. You may use and disseminate CGD's publications under these conditions.



