Recommended

BRIEF
Cost-Effectiveness of COVID-19 Vaccination in Ethiopia
Key messages
- Vaccination against COVID-19 was found to be potentially very cost-effective, and, at the time of the analysis, represented a good investment for Nigeria given the right vaccine at a good price.
- Vaccine price was a more substantial driver of cost-effectiveness than any other single factor. Differences in the costs of different ways to deliver vaccines appear to matter far less.
- Prioritisation by age, in line with the risk of severe disease and the government’s vaccination strategy, improves cost-effectiveness.
- Deploying viral vector vaccines (similar to AstraZeneca (AZ) and Johnson & Johnson (J&J)) in 2021 could have averted up to 430,000 DALYs over a five-year period, when vaccinating 25 percent of the population but prioritising individuals aged 50 years and older. Using an mRNA vaccine (similar to Pfizer-BioNTech or Moderna) could have provided health benefits approximately 18 percent greater.
- The most cost-effective vaccine options against COVID-19 variants previously seen in Nigeria are low-cost viral vector vaccines (AZ or J&J- like). Vaccines with an overall cost per dose less than 2500 Nigerian Nairas (around US $6) per dose are likely to represent the best value for money for the Nigerian government.
- Most vaccination-related costs are concentrated in the first year of vaccination, with costs at much lower levels between years 2 and 5. In the case of an AZ-like viral vector vaccine, economic costs are estimated to range from $440 million to $480 million in the first 12 months. For mRNA-like vaccines, costs could be over $1 billion in the first year.
Background
COVID-19 has disrupted health systems across the globe. Nigeria reported its first COVID-19 case in February 2020, and, since then, the government has rolled out four vaccines to help control the pandemic—Moderna, Oxford-Astra Zeneca (AZ), Johnson & Johnson (J&J) and Pfizer-BioNTech.
Nigeria set an ambitious goal of vaccinating 40 percent of its over 200 million people before the end of 2021, and 70 percent by the end of 2022. The vaccine rollout was organised into four phases, as shown in table 1. Access to vaccines in Nigeria has been limited, however, and vaccine hesitancy has further slowed down deployment. There is also limited evidence on the comparative clinical and cost-effectiveness of COVID-19 interventions—including vaccination—in the Nigerian context specifically.
Table 1. Summary table of the four phases of vaccine roll out in Nigeria
|
Phases of vaccine roll out |
Targeted population |
|---|---|
|
Phase 1 |
Health workers, frontline workers, COVID-19 rapid response team, laboratory network, police, petrol station workers, and strategic leaders. |
|
Phase 2 |
Older adults aged 50 years and above and those with co-morbidities aged 18 and 49 years of age. |
|
Phase 3 |
States and local government areas with high disease burdens, and those who missed phases 1 and 2. |
|
Phase 4 |
Other eligible populations |
Health Technology Assessment (HTA) is a framework for assessing whether healthcare interventions—including vaccines—offer good value for money and take into account a wide range of considerations. The University of Nigeria Nsukka, the London School of Hygiene and Tropical Medicine, the Center for Global Development, and the Africa Centres for Disease Control collaborated to support key national and regional stakeholders in evaluating the cost-effectiveness of Nigeria’s COVID-19 vaccine strategies using an HTA framework.
Key policy questions
- Which COVID-19 vaccines should Nigeria purchase and how much would it cost?
- How should these vaccines be distributed?
- What age groups should be targeted?
Methodology
To reflect the real-world effectiveness of vaccines and recognise the changing evidence on the efficacy of individual vaccines in different populations against different variants, the HTA focussed on broad vaccine types corresponding with the target vaccines of interest to Nigerian policymakers. Vaccine impact was estimated for viral vector vaccines (AZ-like or J&J-like) and mRNA vaccines (Moderna-like or Pfizer-BioNTech-like). Table 2 describes the base price (ie it excludes freight and other delivery costs), dosing, and baseline efficacy used in our cost-effectiveness calculations.
Table 2. Summary of characteristics used to model each hypothetical vaccine
|
Vaccine |
Base price ($) |
Doses needed |
Efficacy (%) * |
|---|---|---|---|
|
Viral vector vaccine 1 (AZ- like) |
3 |
2 |
75 |
|
Viral vector vaccine 2 (J&J - like) |
10 |
1 |
66 |
|
mRNA vaccine (Pfizer- like) |
19.50 |
2 |
90 |
|
mRNA vaccine (Moderna – like) |
32 |
2 |
90 |
*As defined by the reduction in symptomatic infections for the person inoculated
To estimate the impact of vaccination, we used a pre-existing Susceptible, Exposed, Infectious, Recovered and/or Vaccinated (SEIRS+V) COVID-19 compartmental model produced by the Centre for Mathematical Modelling of Infectious Diseases at the London School of Hygiene and Tropical Medicine and adapted for the Nigerian context. Health outcomes are presented in the form of disability adjusted life years (DALYs) averted. DALYs are a measure that captures years of life lost due to premature mortality, adjusted by time spent with disability or disease. One DALY represents the loss of the equivalent of one year in full health.
While we know that COVID-19 vaccines reduce transmission, it is not clear to what extent. For this reason, we modelled all results in two ways. Our disease model output presumed the vaccines have no benefit in reducing transmission and only help the person vaccinated to avoid symptomatic illness. Our infection model presumed that the efficacy of the vaccines against infection transmission was the same as the efficacy against disease. These should be treated as the upper and lower bounds for the vaccines benefit.
The costs of vaccination and the costs of COVID-19 treatment were included in the analysis, with resource use and unit costs sourced from Nigeria-specific data and relevant international evidence.
We measured value for money in the cost-effectiveness analysis by calculating an incremental cost-effectiveness ratio (ICER): the difference in cost between two interventions, divided by the difference in their effect. The comparator scenario in this study was no vaccination. ICERs effectively tell you how much you are paying for every unit of health benefit. The lower the ICER the more cost-effective the intervention is. In order to judge whether an intervention represents a cost-effective choice, cut-offs (or thresholds) are applied. These thresholds are uncertain, but we have attempted to account for what the health system can afford, by using ‘opportunity cost’ based thresholds by Ochalek et al (2018) which give an indication of the level of health that could be displaced as a result of rolling out an intervention.
The cost-effectiveness analysis assumed a 12-month implementation period for all scenarios and delivery strategies (methods for the of delivery vaccines). These delivery strategies were:
- Health facilities - delivery at health centres with adults coming in for vaccination
- Vaccination campaign - temporary delivery at sites other than health facilities, such as town halls, where vaccination is set up for a certain number of days
- Targeted campaign - temporary delivery sites, usually for a day, in sites where people are already congregated, such as places of worship or markets
We modelled costs of delivering AZ-, J&J-, and Moderna-like vaccines across the three strategies, under the assumption that 50 percent of the delivery would take place through facilities, 40 percent through campaigns, and the remainder by means of targeted campaigns. We modelled the costs of delivering the Pfizer-like vaccine only through health facilities.
Key findings
Policy question 1: Which vaccines to buy and at what cost?
The COVID-19 vaccines evaluated can be highly cost-effective (against no vaccination), although important drivers are the cost per dose and the age groups prioritised for vaccination. The analyses did not look at the wider economic benefits of COVID-19 vaccines, such reducing the need for lockdowns, but these effects would have likely further improved the value for money of these vaccines.
Vaccination with viral vector vaccines (AZ-like or J&J- like) could avert up to 430,000 DALYs over a five-year period, when vaccinating 25 percent of the population but prioritising individuals aged aged 50 years and older. However, using an mRNA vaccine (similar to Pfizer-BioNTech or Moderna) could have provided health benefits approximately 18 percent greater.
From the point of view of the Nigerian healthcare system, and the resources available to it, the viral vector vaccines (AZ-like or J&J- like) may represent optimal choices.
Vaccine price has a considerable impact on cost-effectiveness. Consistent with other similar evidence, to remain cost-effective in Nigeria, vaccination costs should not exceed around $6 per dose. Vaccines priced at a level to achieve that cost per dose compared favourably with other interventions that could be provided within the health budget (see figures 1 and 2). In other words, the viral-vector based vaccines tended to fall below thresholds that more realistically reflect what the health service could pay for. Moreover, some of our analyses indicated that these vaccines could provide health benefits at lower overall costs (taking into account savings from COVID-19 related treatment and management), leading to negative ICERs.
Most vaccination-related costs (excluding any potential savings from reduced treatment) are concentrated in the first year of vaccination, with costs at much lower levels between years 2 and 5. In the case of an AZ-like viral vector vaccine, economic costs are estimated to range from $440 million to $480 million in the first 12 months. For mRNA-like vaccines, costs could be over $1 billion in the first year.
Figure 1. Cost-effectiveness plane indicating cost per DALY estimates for the scenario where 25 percent coverage of all adults (prioritizing 50+ years of age) are vaccinated. In this analysis it is assumed that vaccination would impact on disease only, with no impact on infection, but with reduced onward transmission. The dotted lines indicate the cost-effectiveness thresholds used.
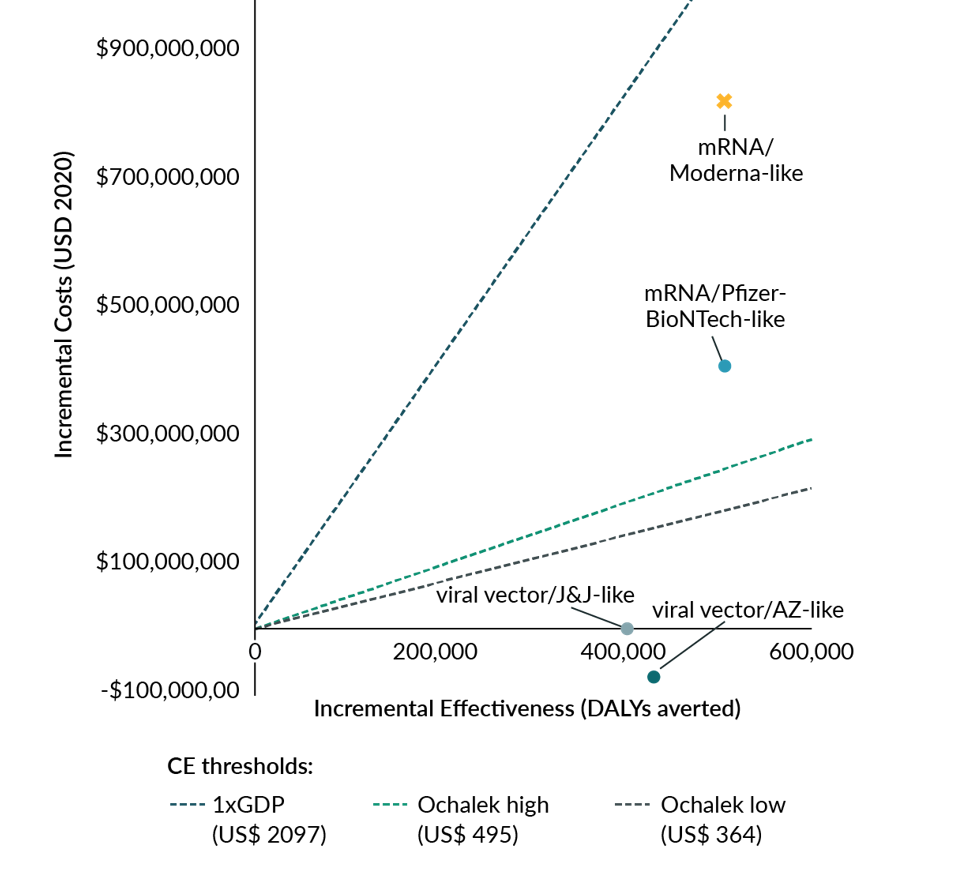
Figure 2. Cost-effectiveness plane indicating cost per DALY estimates for the scenario where 25 percent coverage of all adults (prioritizing 50+ years of age) are vaccinated. In this analysis, it is assumed that the vaccines prevent infection (and thus disease), but with no impact on breakthrough disease. The dotted lines indicate the cost-effectiveness thresholds used.

Policy question 2: How should the vaccines be distributed?
Costs for each of the delivery strategies (campaign, targeted campaign, health facility) differ only slightly and do not appear to impact on relative cost-effectiveness (See table 3). However, the study did not include the impact of potential implementation constraints, particularly with respect to human resources, of a very rapid roll-out. This may be particularly important for high coverage scenarios.
Policy question 3: What age groups to target?
Cost-effectiveness is strongly associated with the risk of severe outcomes of the person vaccinated. Accordingly, targeting people aged 50 years and over was more cost-effective than targeting 18-49-year-olds (See table 4).
Table 3. Analysis of the impact of delivery methods on cost-effectiveness. Results shown only for Moderna-like and AstraZeneca-like vaccines. Assumptions: 25 percent coverage of adult population, prioritising aged 50+
|
Vaccine mechanism: disease |
|||||
|---|---|---|---|---|---|
|
Vaccine type |
Delivery method |
Cost per dose |
Total costs (millions) |
Total DALYs averted |
ICER |
|
Viral vector (AZ-like) |
Health facility |
$6.19 |
$38.0 |
219,359 |
$174.10 |
|
Campaign |
$7.12 |
$60.9 |
219,359 |
$278.57 |
|
|
Targeted campaign |
$7.08 |
$59.9 |
219,359 |
$274.07 |
|
|
mRNA (Moderna-like) |
Health facility |
$44.24 |
$946.1 |
267,707 |
$3,538.02 |
|
Campaign |
$45.16 |
$968.7 |
267,707 |
$3,622.47 |
|
|
Targeted campaign |
$45.13 |
$968.0 |
267,707 |
$3,619.71 |
|
Vaccine mechanism: infection |
|||||
|---|---|---|---|---|---|
|
Vaccine type |
Delivery method |
Cost per dose |
Total costs (millions) |
Total DALYs averted |
ICER |
|
Viral vector (AZ-like) |
Health facility |
$6.19 |
-$88.2 |
429,601 |
-$207.82 |
|
Campaign |
$7.12 |
-$65.3 |
429,601 |
-$153.93 |
|
|
Targeted campaign |
$7.08 |
-$66.3 |
429,601 |
-$156.25 |
|
|
mRNA (Moderna-like) |
Health facility |
$44.24 |
$803.4 |
504,283 |
$1,581.33 |
|
Campaign |
$45.16 |
$826.1 |
504,283 |
$1,626.26 |
|
|
Targeted campaign |
$45.13 |
$825.3 |
504,283 |
$1,624.79 |
Table 4. Strategies which prioritised older age groups were more cost-effective (relative to no vaccination) than a strategy focused on vaccinating 90 percent of those aged 18 and above. Data presented for the viral vector vaccine (AZ-like) only.
|
Vaccine mechanism: disease (Viral vector – AZ-like) |
|||
|---|---|---|---|
|
Scenario |
Total costs (millions) |
Total DALYs averted |
ICER |
|
25% adults (prioritise 50+) |
$49.3 |
219,359 |
$224.99 |
|
100% 50+ |
$17.1 |
105,792 |
$162.33 |
|
90% adults |
$240.0 |
419,026 |
$572.80 |
|
70% 50+ |
$36.9 |
142,580 |
$259.04 |
|
70% 50+, 25% 18-49 |
$87.2 |
226,197 |
$385.72 |
|
Vaccine mechanism: infection (Viral vector – AZ-like) |
|||
|---|---|---|---|
|
Scenario |
Total costs (millions) |
Total DALYs averted |
ICER |
|
25% adults (prioritise 50+) |
-$76.9 |
429,601 |
-$178.96 |
|
100% 50+ |
-$31.9 |
194,811 |
-$164.25 |
|
90% adults |
$83.5 |
679,467 |
$122.90 |
|
70% 50+ |
-$33.4 |
268,114 |
-$124.43 |
|
70% 50+, 25% 18-49 |
-$91.0 |
526,873 |
-$172.72 |
Conclusions
COVID-19 continues to present new challenges, with novel variants emerging with unpredictable consequences for vaccine effectiveness. Nevertheless, the current analysis showed that COVID-19 vaccines—especially the viral vector vaccines—have significant benefits, and represent cost-effective choices from a Nigerian health sector perspective. However, based on the current evidence, it is important that vaccines do not exceed $6 dollars per dose. Policymakers in Nigeria should prioritise lower-cost doses and, where possible, negotiate with pharmaceutical companies to secure affordable prices.
The results have broadly confirmed the age group prioritisation strategy of the Nigerian government, which focused on a 50+ cohort during phase 2 of the rollout.
The costs for each of the delivery strategies (campaign, targeted campaign, health facility) differ only slightly and do not appear to impact on relative cost-effectiveness. It is better for the choice of delivery strategies to be guided by programmatic and resource capacity rather than cost-effectiveness concerns.
Given the recent emergence of the COVID-19 Omicron variant, analyses may need to be updated where a new variant substantially changes the nature of the disease.
Acknowledgements
We would like to thank the organizations and professionals involved in this study. Our special thanks go to the Nigerian Federal Ministry of Health and the National Primary Health Care Development Agency, for their inputs and support of this work; Dr Justice Nonvignon and Dr Elias Esfaw at Africa CDC for their inputs into this project; Dr Tom Drake at CGD for his support and overseeing iDSI’s series of vaccine HTA projects.
Topics
CITATION
S.C. Uzochukwu, Benjamin, Chinyere Okeke, Sergio Torres-Rueda, Carl Pearson, Eleanor Bergren, Anthony McDonnell, Anna Vassall, Mark Jit, and Francis Ruiz. 2022. Understanding the Cost-Effectiveness of COVID-19 Vaccination in Nigeria. Center for Global Development.DISCLAIMER & PERMISSIONS
CGD's publications reflect the views of the authors, drawing on prior research and experience in their areas of expertise. CGD is a nonpartisan, independent organization and does not take institutional positions. You may use and disseminate CGD's publications under these conditions.



