Recommended

The global COVID-19 pandemic has highlighted the pressing need to improve oxygen supplies around the world. Recent waves across South America, South Asia, and Africa have caused surging oxygen demands and revealed tragic scenes of oxygen shortages and stock outs. In February 2021, belatedly, international organisations under the Access to COVID-19 Tools Accelerator Therapeutics pillar launched the COVID-19 Oxygen Emergency Taskforce. Countries can now seek support for oxygen scale-up from these organisations, including the Global Fund’s large $3.5Bn COVID-19 Response Mechanism (CRM). Countries have an opportunity to apply for support from the CRM in May and June 2021 in the first instance, and indeed the CRM has recently approved $US75 million for India.
In this blog, we highlight key objectives that countries need to consider in their funding applications for support from the CRM for the successful scale up of oxygen and critical care. Firstly, we propose that in addition to seeking funding for improving oxygen supply and distribution, countries should take advantage of the CRM to request funding and technical assistance for the scale up of healthcare and clinical routines required to use oxygen effectively. Secondly, since oxygen is highly constrained in most low- and middle-income country (LMIC) health systems, it is vital to define an essential set of interventions that are cheap, effective, scalable, sustainable, and accessible for critically ill patients even after the CRM ends. We outline such a package of expert-defined Essential Emergency & Critical Care (EECC) from our research that countries can use in their CRM submissions.
Patients need more than a scale up of oxygen supplies, and the CRM can support the essential care necessary to make oxygen use effective
There have been many reports from countries like India, Brazil, and Nepal where severe or critical COVID-19 patients have not been able to access oxygen or critical care. In response, the media has rightly focused on the need to scale up oxygen production and oxygen distribution infrastructure in recent COVID-19 waves. However, the basic, life-saving clinical processes that accompany oxygen provision are often overlooked in settings of both high and low resources, as people tend to focus on medical equipment and high-end care such as oxygen concentrators and ventilators.
When a patient has symptomatic COVID-19, the patient’s airway, breathing, or circulation may become compromised, and early identification of the problem and timely care can be lifesaving. However, simple equipment (e.g. pulse oximeters), consumables, drugs, staffing, and routines for early identification and timely critical care is often missing, and guidelines may be too specialised or not context-appropriate. Without these critical care measures, the effectiveness of scaling up oxygen will be very limited.
To improve outcomes for seriously ill patients that can be delivered in all hospital settings, the Essential Emergency and Critical Care concept was devised. EECC is defined as the care that should be provided to all critically ill patients in all hospitals worldwide. Importantly, it is about strengthening the basics, and stands in stark contrast to advanced critical care, represented by ventilators and dialysis units, that are expensive, difficult to provide at the scale needed, and are not necessary (or may even be harmful) for many critically ill patients.
In one recent project, we worked with clinical experts from high-, middle- and low-income countries to reach a consensus on the content of EECC – the essential care necessary for all critically ill patients. The project was carried out by a team of international researchers and funded by the Wellcome Trust. It included 272 clinical experts from 59 countries worldwide in a Delphi consensus methodology. Agreement was reached on 40 clinical processes and 67 hospital resources necessary for the essential care of all critically ill patients. These include, for example: monitoring basic vital signs to identify critical illness; provision of oxygen therapy and intravenous fluids; and positioning of unconscious patients to maintain a free airway. Additional processes and resources were agreed for the specific care of critically ill patients with COVID-19.
Focusing funding (and oxygen) on the most cost-effective COVID-19 care
Although the CRM represents an expansion of international funding for oxygen supplies (and in addition there is World Bank funding and UNICEF’s $US182 million Supplies Facility Fund), the scale of future waves in most LMICs are likely to outstrip this additional provision.
Our initial analysis in Kenya suggests that cost per patient, per day for severe COVID-19 disease managed in general hospital wards and those with critical COVID-19 disease admitted in intensive care units are US$125 and US$600 respectively. During a large wave this could consume a large amount of health resources and more importantly, it could rapidly deplete available oxygen supplies, as has been shown vividly in India. Therefore, it is vital for proposals to the CRM to consider how to get the most health impact for the limited amount of oxygen available. Technical Review Panels (TRPs) should support proposals that focus on the most efficient, equitable, and scalable package of care to fund.
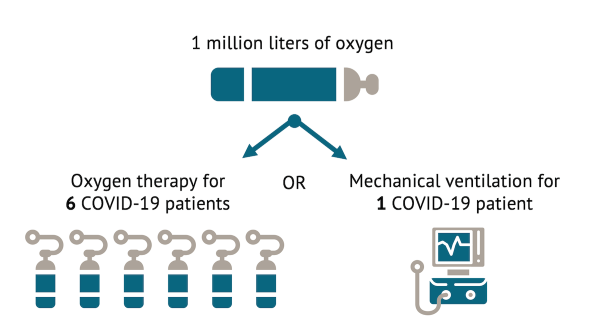
In their CRM submission, countries will need to choose the appropriate balance between ventilator scale up versus scaling-up simple oxygen therapy, combined with appropriate patient support and monitoring in the form of EECC. They will also need to consider feasibility and timeliness given limited system capacity and the long lead time in scaling up ventilator-based care. We will be reporting formal estimates of the comparative cost-effectiveness later in the year, but based on WHO guidelines, ISARIC time in therapy data and our initial research, a ventilated patient consumes at least six times more oxygen than those who require simpler oxygen therapy (see figure 1). When oxygen is highly constrained, such as at the peak of a COVID-19 wave, expanding ventilator access may therefore have unintended harmful opportunity costs on the care of other patients.
Figure 1. Comparison of per patient consumption of oxygen for oxygen therapy versus ventilators
Countries could choose to focus on the scale-up of the EECC package of care. Using the CRM to expand this focused set of interventions has the potential to save the lives of COVID-19 patients, and also be useful for other diseases now and in the future, including TB, HIV, and malaria. Preliminary findings from our work show that treating a severely ill covid patient with EECC in Tanzania could cost 20-25 USD per day. Drivers of the total cost includes oxygen provision (38%) and will be dependent on the required length of stay in hospital. Optimised care using standard routines and guidelines that can reduce the length of stay and ensure careful management of oxygen may further increase the value for money of COVID-19 care and ensure limited oxygen supplies are used most efficiently.
Recommendations
The Global Fund CRM is an excellent opportunity for countries to seek funding for both oxygen scale up, and the essential package of care needed to minimise COVID-19 deaths. Countries and TRPs looking to maximise the value for money of CRM proposals should consider the balance between advanced and essential critical care and whether enough support has been requested to deliver oxygen and EECC effectively to COVID-19 patients. Attempts to scale-up mechanical ventilation (or advanced critical care) is likely to have high opportunity costs during the peak of the pandemic, given its large resource requirements including trained human healthcare resources and the high consumption of oxygen. The EECC package can be used by countries and TRPs to help ensure applications are high impact and will produce sustainable benefits for health systems and patients through and after the pandemic.
DISCLAIMER & PERMISSIONS
CGD's publications reflect the views of the authors, drawing on prior research and experience in their areas of expertise. CGD is a nonpartisan, independent organization and does not take institutional positions. You may use and disseminate CGD's publications under these conditions.


{kind=link}