Recommended

Blog Post

CGD NOTE
USAID’s Family Planning and Reproductive Health Program
Last week, USAID’s Global Health Bureau launched an event “Maternal and Child Survival: A Decade of Progress and Action for the Future”, cohosted by UNICEF, the governments of India, Senegal, and the United Kingdom, which was livestreamed globally. A congressional factsheet and strategic framework, infographic, and results snapshot were released (see here for more details). The event follows up from a USAID-hosted event 11 years ago (which we at CGD also followed—see here).
In this piece, I recap a few key messages on USAID’s call to action, honing in on the role of data and evidence in driving policy and decision-making. I argue that we need better data on the progress of maternal and child survival through improved health information systems as well as greater use of economic evidence to help drive priorities. These two approaches can help donors and governments drive reductions in preventable deaths of moms and babies.
Use data on progress and return on investment for policy decisions
The speeches by all the global health leaders used data to make the investment case:
- USAID assistant administrator of global health Atul Gawande stated that we had “lost sight of the survival of children and women because of (the) pandemic. We have to rebuild that momentum.”
- USAID administrator Samantha Power noted in her keynote: “The momentum of the early 2000s has at best plateaued from 2016 to 2020. Maternal mortality rates virtually flatlined. Under-five mortality rates which declined by double digits every five years since 2000 also slowed.”
- WHO executive director Tedros Adhanom remarked: “We’re severely off course in meeting the Sustainable Development Goal for reducing maternal mortality... Similarly, more than 50 countries are not on track to achieve the 2030 newborn and child survival targets.”
- Catherine Russell, UNICEF’s executive director, argued that: “investing in the health and nutrition of women, children and adolescents offers a ten-fold return including through better educational outcomes, workforce participation, and social contributions.”
Improve routine data systems on maternal and child mortality
While all policymakers agree on the importance of using data to track reductions in maternal and child mortality, the ability to report on mortality requires underlying data systems for health surveillance. Most people zone out at the mention of “data systems” or “health surveillance”, but since we all agree on the importance of the numbers, then we should agree that the underlying systems that collect and report such data are crucial as well. These numbers do not come out of thin air—nor out of analytical machinery from Geneva or Seattle.
Fortunately, the US government is arguably one of the most important investors in health information around the world. Through USAID’s investments, the Demographic and Health Surveys, a $200 million contract awarded over 5 years, is a crucial underlying source of data on child and maternal mortality for low- and middle-income countries (LMICs). But these data sources should complement, rather than substitute, routine health information systems (RHIS) and civil registration and vital statistics systems (CRVS), not to mention the need for coordination with other international surveys such as the UNICEF Multiple Indicator Cluster Survey, which also measures similar indicators for child health.
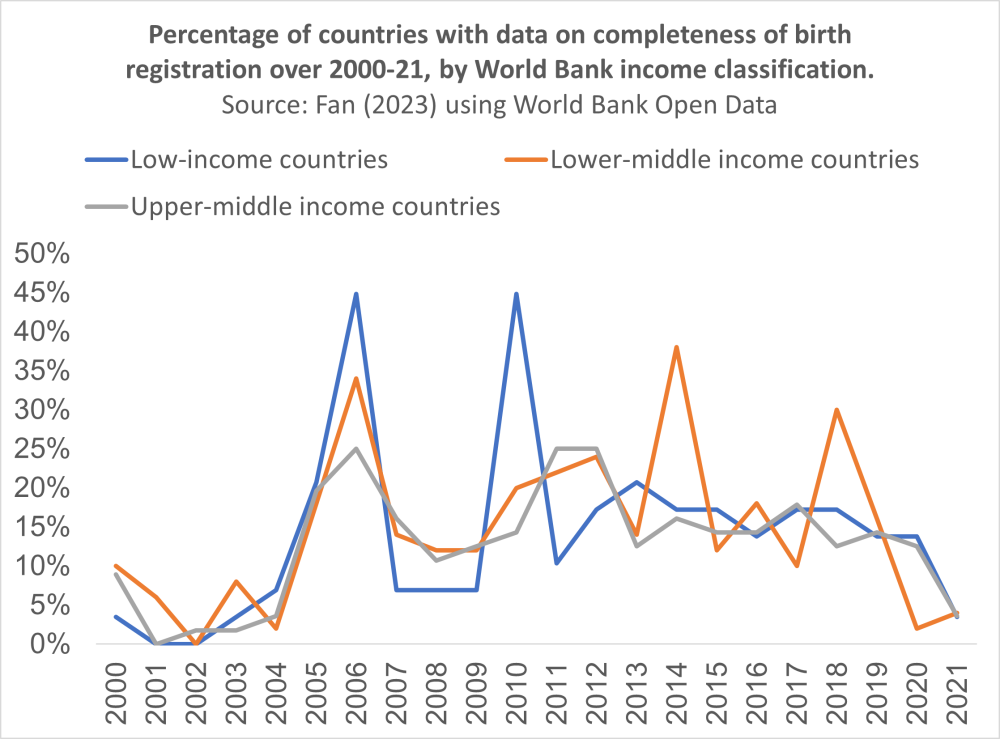
I argue that investments in maternal and child health should not only support these surveys, but also spur improvements in core data systems (RHIS, CRVS) which are typically administered by health or statistics ministries. Whether data systems are improving can be measured by data on the completeness of birth registration and death registration, indicators which are reported largely by UNICEF. Regrettably, over the two golden decades of global health, the completeness and quality of key birth and death data have likely stalled.
Unfortunately, attempts to track whether countries are building stronger data systems has not been prioritized by the global health community and its constellation of funding agencies. It’s challenging to say whether there has been progress in completeness of birth coverage, a key indicator of the quality of a country’s CRVS. A time series of completeness of birth coverage by country is not even possible, as most countries have not been reporting this indicator over time.
In analyzing the World Bank Open Data indicator on completeness of birth coverage, I counted the percentage of countries which reported data for this indicator, clearly showing that policy priority and attention to reporting on birth registration completeness has been stagnating or in decline. It’s not been a global priority, even as the push for data and evidence-based policy making in DC and Geneva have grown.
What’s measured is what gets done. If completeness of birth registration is not being measured, it’s likely not improving.
How then, you may ask, are we able to report on reductions in maternal and child mortality? Here comes the rub—or rather the analytical machinery producing the so-called Global Burden of Disease estimates by the Institute for Health Metrics & Evaluation and the World Health Organization (WHO) (see here for my past blog on malaria estimates for example).
While these synthetic data are valuable, there is no substitute for underlying data collection. We also do not know the extent of the imputation (read: guessing numbers for countries for which there is no data) and whether that has decreased over time from these institutions based in Seattle or Geneva. The percentage of estimates which are imputed should be a critical indicator of the quality of synthetic data prepared by the WHO and IHME for the GBDs. The bandied statistic that the original 1994 GBD extrapolated for all world deaths using 1 percent of the world’s mortality data should have increased, but we just don’t know.
Perhaps most concerning is that the global production of death estimates at country level by Geneva or Seattle hides the quality of underlying data. What’s worse is that such multi-million dollar institutional efforts in the North may risk reinforcing incentives to not improve data quality and death registration in the South. Despite the two golden decades of global health, certain global health circles cite unproven claims of system-wide spillovers due to vertical initiatives in HIV, tuberculosis, malaria—and yet the stagnation in maternal and child survival should be cause for concern about negative spillovers of highly disease-focused vertical initiatives. We need to ask whether the global health community has strengthened the basics of public health infrastructure and health systems in countries around the world. As the world addresses COVID-19 concerns to improve pandemic preparedness and surveillance, the same problems of underlying data systems need to be addressed. We need to renew an emphasis on horizontal systems of care.
In my conversation with health information systems experts, I have heard horror story upon horror story of duplicative pilot health information systems funded by siloed global health donors. In an anecdote for one African country, there were more than 70 fragmented health information systems. The “e-Chaos” from endless duplication is bad value for money and waste, littering a graveyard of junk digital products with no sustaining system improvements in data quality and coverage to speak of. Countries and donors need to better align investments, by focusing on a comprehensive and inclusive information system.
In contrast, one could argue that PEPFAR’s highly focused attention to reporting coverage of antiretroviral therapy to the US Congress helped to drive improvements in country data quality on HIV. While the quality of maternal and child health data in RHIS is likely to lag that of HIV, we just don’t know. Indeed, in my past analyses of the World Health Statistics found great variation in reporting of indicators by disease, which are likely driven in part by demands by donors (perhaps a plucky graduate student or the WHO has interest to update this work as well).
Who cares about data governance in health? Work by the Health Data Collaborative (which arguably succeeded its predecessor the Health Metrics Network—a $50 million initiative that shut down unceremoniously), the WHO’s Data, Analytics and Delivery team, and Bloomberg Philanthropies to strengthen data for health are helping to advance this cause of data for health. Perhaps it’s a tad ironic that tech moguls that turned into global health moguls have had little concern in IT infrastructure, software and data systems in LMICs. Meanwhile, Health IT arguably remains at the fringe rather than the center of global health policy attention, even as statistics and metrics of global health are top of mind. Much more policy attention is needed on data for health if we hope to see improvements in maternal and child health.
Use priority setting and cost-effectiveness to make strategic health investments
Just as UNICEF’s Catherine Russell referred to cost-benefit analysis of investing in maternal and child health to make the case, so too would the maternal and child health community, including USAID, benefit from greater use of economic evidence on the value of interventions. Such evidence helps to make the case to both donors and national policymakers, such as ministries of finance. Fortunately, under Samantha Power’s leadership in establishing the office of the chief economist, the potential for USAID to use economic evidence is arguably greater than ever before.
This year also marks the 30th anniversary of the 1993 World Development Report (WDR), which pioneered the use of cost-effectiveness in identifying a highly-cost effective package of interventions. The 1993 WDR was also instrumental in inspiring Bill Gates in investing in global health, because saving lives could be so cheap and cost-effective. Since then, the 1993 WDR has gone through two successive editions of the Disease Control Priorities: DCP2 (the 2006 second edition) as well as DCP3 (the third edition which comprised of nine volumes).
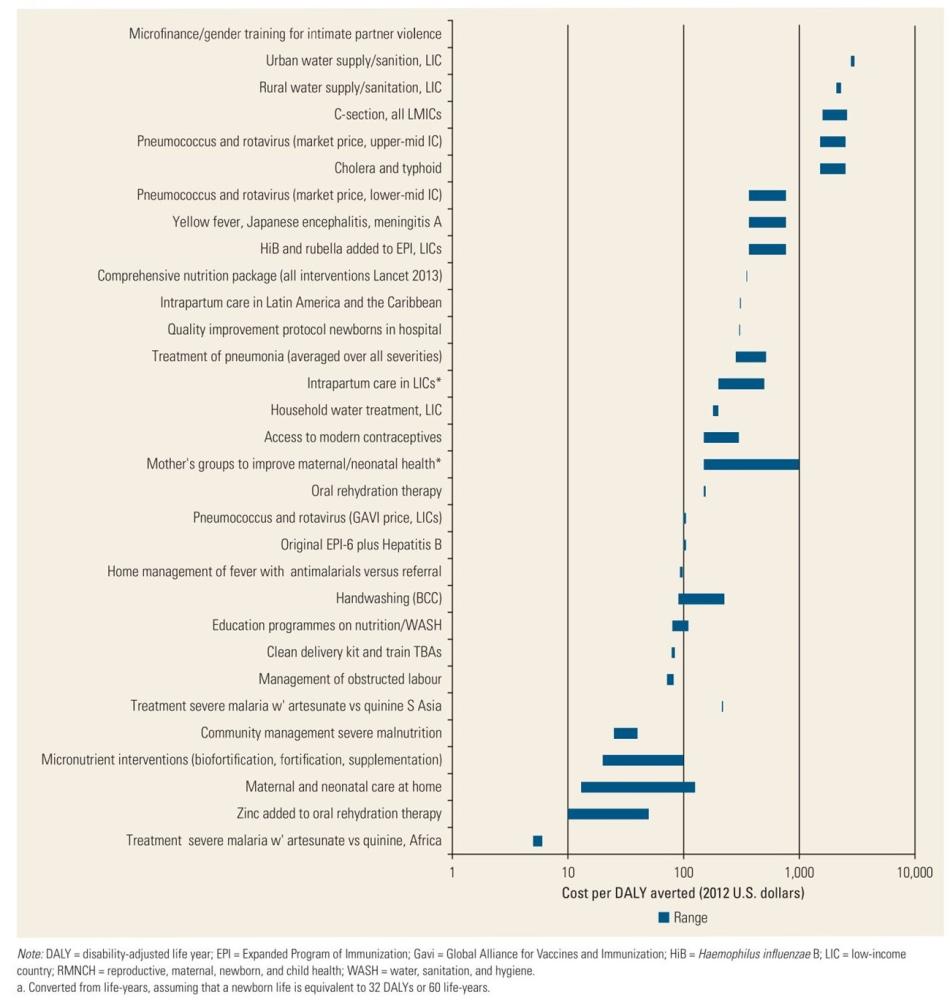
I returned to the DCP3 volume on reproductive, maternal, neonatal, and child health investments, and the cost-effectiveness chapter (see here and figures below). The evidence is clear that investments in reproductive, maternal, neonatal, and child health are highly cost-effective, ranging from less than $10 USD per DALY averted for treatment of severe malaria (2012 terms), to more than a $1000 USD per DALY averted for C-section. Since then, there should be many more interventions, innovations, and evaluations about the impact and cost-effectiveness of what works to improve maternal and child survival.
The Center for Global Development too has been long focused on impact evaluation (see here and here) and priority setting in global health (see here, here, here, and here), which champions the use of evidence and cost-effectiveness in particular in driving decision-making. CGD’s recent work in priority setting, through the International Decision Support Initiative, has incubated a global facility to help countries to institutionalize priority setting—that countries should build local priority setting institutions that help to generate evidence and collect data about what works and at what cost.
There is no easy way to develop local institutional capacity for science and evidence. As part of the global health community, we should imagine how to build organizations and institutions through strategic investments, not merely rely on external private contractors. We should not only invest in things which we know work; but also in the systems that help us to innovate and learn what works. I would argue that the faster we can shift to local institutions for local evidence and data, the faster that countries can learn and improve on their own.
With thanks to Vikas Dwivedi, Amanda Glassman, Javier Guzman, the Health Data Collaborative, and others for helpful comments.
Figure. Cost-Effectiveness of Interventions for RMNCH in 2013 USD per DALY averted from DCP3 (originally figure 17.1 in the chapter)
Topics
DISCLAIMER & PERMISSIONS
CGD's publications reflect the views of the authors, drawing on prior research and experience in their areas of expertise. CGD is a nonpartisan, independent organization and does not take institutional positions. You may use and disseminate CGD's publications under these conditions.
Thumbnail image by: Adobe Stock



