Recommended

Hundreds of millions of dollars are typically spent developing a new vaccine. You would assume that by the time the vaccine receives approval, we would know precisely the right dosing regimen: how much vaccine to give, how many doses to administer, and the best spacing between them. But that’s rarely the case.
Rather, vaccines that reach the market are often far from optimal. Yes, newly approved vaccines are safe and effective, but they are not always optimized to reach as many people, save as many lives, and stretch budgets as far as possible. A new CGD policy paper, released today, explores why this happens and argues that optimizing vaccine regimens is a high-impact—and often overlooked—opportunity in global health.
Take the human papillomavirus (HPV) vaccine. For years after its introduction, countries administered it as a three-dose series. Then additional evidence emerged; eventually, a single dose proved to be non-inferior. This policy shift, driven by updated World Health Organization (WHO) guidance, has been a game-changer—massively reducing delivery costs while expanding coverage in low- and middle-income countries (LMICs). But it took 16 years from regulatory approval to WHO recommendation. Had this change been implemented just five years earlier, the paper estimates that 150,000 lives could have been saved. Although this case is just an illustrative calculation, it demonstrates the scale of the missed opportunity.
Yet, despite the potential for significant benefits, the current paradigm of vaccine development and delivery does not provide strong incentives for optimization. Often, decision makers treat approved vaccines as fixed entities. But with tighter budgets and an ever-expanding menu of available vaccines, the case for optimization is more urgent than ever.
Why optimization matters, and why it’s hard
Many aspects of vaccination programs can be optimized. Countries deciding which vaccines to use in routine vaccination programs is one important example. But the paper focuses on a particular kind of optimization that is arguably underexplored: adjusting the number of doses, the size of each dose, or the spacing between multiple doses.
We have seen this type of optimization in many public health emergencies and cases of vaccine shortages. Beyond HPV, recent examples include increasing the gap between doses of COVID-19 vaccines, decreasing doses of mpox vaccine in the US, and controlling yellow fever outbreaks in the Democratic Republic of the Congo. All these examples have successfully stretched limited vaccine supplies.
While in some cases public health may require switching to more, not fewer, doses to sustain population protection (measles and varicella in the US are notable examples from the past), the decreases are more common and offer very important public health benefits, because they stretch limited supplies and budgets. This could have substantial benefits for LMIC governments and global immunization partners, such as Gavi, all of whom are currently navigating tough fiscal realities. It could also help pave a more sustainable transition pathway from Gavi support by ensuring countries eventually have to self-finance more affordable vaccine portfolios.
However, the historical examples of past successes should not distract from the slow and inconsistent nature in which optimization is currently implemented. For example, the paper argues that for the COVID-19 vaccine manufactured by Moderna, half of the original dose could have been considered—as was eventually implemented for boosters in the winter of 2021—and that doubling its supply in that period could have saved 250,000 to 500,000 lives. (If this strikes readers as a very large number, note that this reduction is less than 10 percent of the total number of lives that were estimated to have been saved by COVID-19 vaccinations in 2021.)
Optimization is challenging due to a range of barriers and market failures. The paper explores the incentives and disincentives facing each stakeholder in more detail, but to simplify, we could see them as both supply-side and demand-side failures.
First, on the supply side, vaccine producers are incentivized to demonstrate efficacy and be the first to reach the market. Investigating lower-dose regimens or alternate dosing schedules may be scientifically valuable, but this is rarely a commercial priority. And the high cost of R&D is itself a key barrier to more experimentation.
Second, on the demand side, even when optimized regimens become available, uptake by countries is low. Slow adoption is often due to information asymmetries, policy inertia, and delivery constraints. Each decision to change dose is mediated by regulatory agencies (for label changes) and national immunization advisory boards and WHO (for off-label use), with each actor facing a different set of priorities—and often disincentives to depart from the status quo.
Two high-impact opportunities for optimization
While the optimization agenda covers many vaccines (i.e., ones that are already-approved and those in development), we see two concrete, high-impact opportunities on the horizon:
- The pneumococcal conjugate vaccine (PCV) is already Gavi’s top cost driver, consuming $1 billion of its 2026–2030 budget. But new WHO SAGE guidance, from March 2025, suggests that in countries with consistently high coverage (≥80–90 percent over five years), either one of three shots could be dropped, or each of the three doses can be lowered to 40 percent of the standard dose. While implementation requires sufficient epidemiological surveillance, its cost would be offset by significant savings in vaccine costs: a retrospective analysis suggests that for the 2020–25 period this approach could have led to as much as $250 million in savings.
- New tuberculosis vaccines, currently in phase 2–3 trials, are another high-impact example. Given initial promising results, a future vaccine could prove highly effective, but may also become a significant cost driver for countries and/or Gavi—and optimization may prove highly beneficial both in terms of health and economic value.
Why Gavi should take a more proactive role
Gavi is uniquely positioned to play a leading role in advancing the vaccine optimization agenda, alongside partners like WHO, CEPI, and UNICEF. It is an area that aligns closely with Gavi’s 6.0 strategic focus; strengthening “countries’ prioritization and optimization of vaccine programmes” is listed as the top goal under the new strategy.
This marks a shift from Gavi’s previous strategy, which referenced optimization to a somewhat narrower extent. Whereas previous iterations have treated vaccines as fixed inputs, those that could be delivered faster, targeted better, and bought more cheaply, the 6.0 (i.e., 2026–2030) strategy signals a greater emphasis on optimizing what vaccines are delivered—not just how they are targeted and delivered.
“The Alliance will offer a wider range of vaccines in a fiscally constraint environment. It will be critical to support countries optimise their existing vaccine portfolios and prioritise and target the introduction and scale up vaccines that are most appropriate for their local context, capacity and based on evidence.”
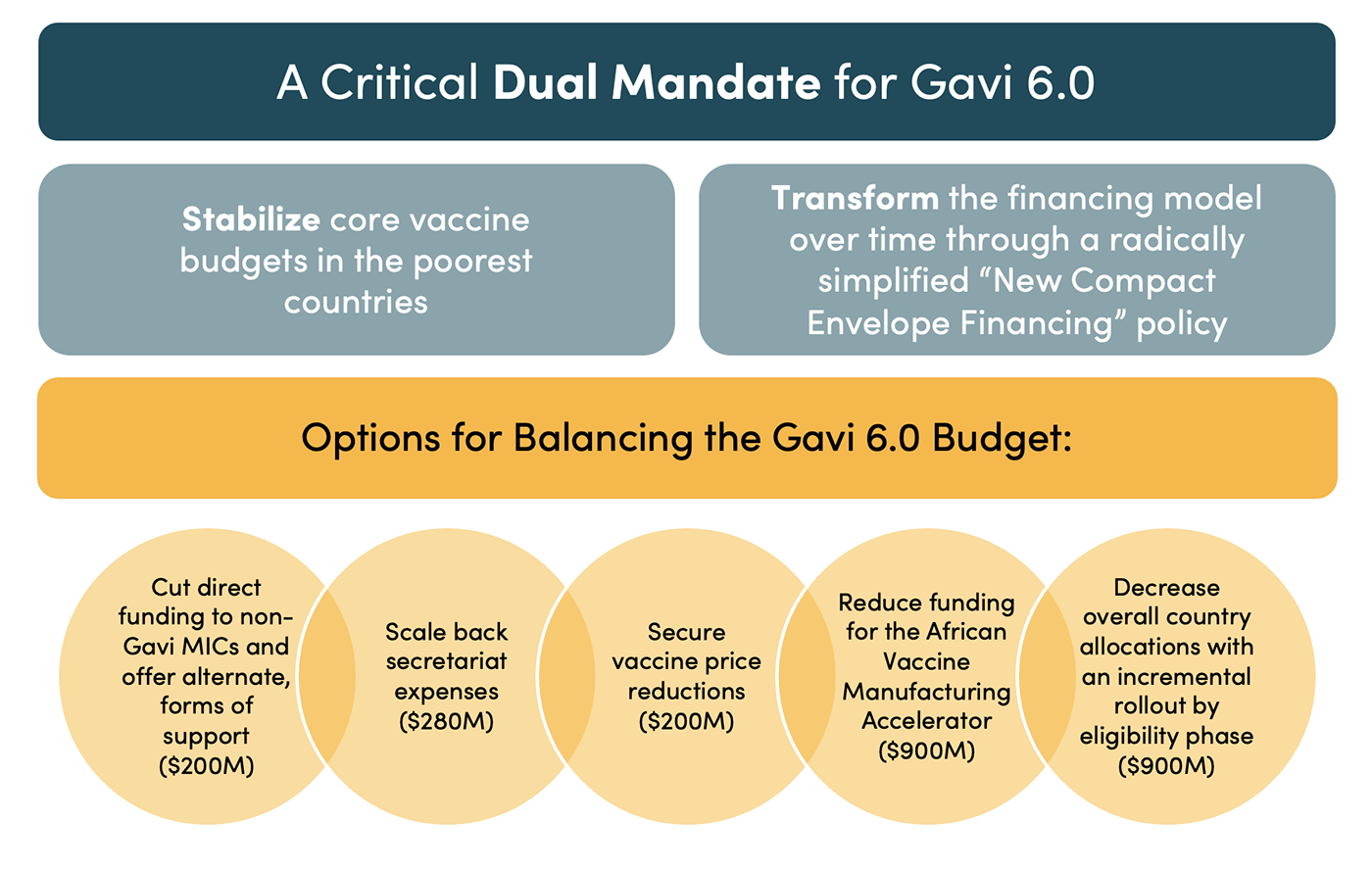
This shift comes at an opportune time. The “portfolio” of vaccines supported by Gavi is now larger than ever. Gavi is facing a $3 billion budget shortfall over the next five years, and LMIC health budgets are under immense fiscal pressure. For 6.0, Gavi is also evolving its funding model by consolidating vaccine support and programmatic cash support into a single “envelope” for each country, with the aim of promoting greater country autonomy in decision making. Vaccine optimization—not just of which vaccines to use, but also how to use them—should be part of this transition.
Policy options to prioritize vaccine portfolio optimization
Any decisions about vaccine optimization, either at the country or international level, hinge on the availability of evidence. Therefore, an effective optimization agenda encompasses both evidence generation and acting upon that information. Here are two ideas for how Gavi should play a larger role in the optimization agenda going forward. In both cases, a potential target for these considerations could be the upcoming TB vaccine.
- Option 1: "Push” funding. By “push” we mean unconditional funding of vaccine dosing research, for example via grants to existing research organisations. Two major funders currently support optimization research: the Gates Foundation and the US National Institutes of Health. The Gates Foundation has set a sunset date of 2045, meaning its research agenda could likely be increasingly focused on projects that yield impact in the near future. Since it can typically take five to ten years to generate evidence needed for optimization, there is a risk that funding from Gates could gradually decrease. And future funding for vaccine research from the NIH is highly uncertain. In this context, there is a need for a new funding source—or consortia/partnerships—that could pursue a comprehensive, long-term vaccine optimization agenda, ideally in a way that is closely aligned with Gavi’s strategic targets.
- Option 2: “Pull” funding. By “pull” we mean funding which is conditional on outcomes of research. Gavi could lean into its comparative advantage in market shaping and play a key role in incentivizing more optimization in two ways: 1) Prizes or milestone funding that could spur further research into optimization by rewarding the discovery of more efficient dosing regimens; and/or 2) tying procurement to credible dose-response data. This mirrors AMC-style pull funding proposed by our colleagues at the Market Shaping Accelerator for repurposing of drugs—paying more (or ranking bids higher) when producers deliver verifiable evidence on dosing. That way firms face a clear incentive in the form of a reward for generating data on optimal dosing of vaccines.
The choice of whether to use “push” or “pull” funding will depend on how well the funder(s) can identify which organization is best equipped to undertake optimization research and how clearly they can define the desired results. For example, “push” funding models are best-suited when a funder can identify the firm/organization best positioned to undertake research and generate evidence: often the original developer, who has the technical expertise and can conduct this research early in the development cycle, when otherwise there is little commercial incentive.
On the other hand, “pull” funding models are useful when researchers or companies have information that funders cannot easily observe. For some of the existing vaccines, pull funding may motivate third parties to generate evidence.
Conclusion
Optimization can save lives and reduce vaccine costs, benefiting all countries and global immunization partners like Gavi. It also offers a critical insurance mechanism for vaccines facing supply shortages, especially pandemic vaccines. But the lack of incentives to generate the required evidence for it poses a major barrier. Gavi and its partners should seize the opportunity to accelerate evidence generation and make more proactive decisions about when to optimize. Doing this would help Gavi realize fiscal savings and maximize health impacts. It would also benefit countries that are no longer or never were eligible for Gavi support.
DISCLAIMER & PERMISSIONS
CGD's publications reflect the views of the authors, drawing on prior research and experience in their areas of expertise. CGD is a nonpartisan, independent organization and does not take institutional positions. You may use and disseminate CGD's publications under these conditions.
Thumbnail image by: AMO/ Adobe Stock



