Recommended

POLICY PAPER
How the Global Fund Can Adapt to a Shrinking Aid Landscape

BRIEF
A Radically Simplified Global Fund to Meet the Moment
BRIEF
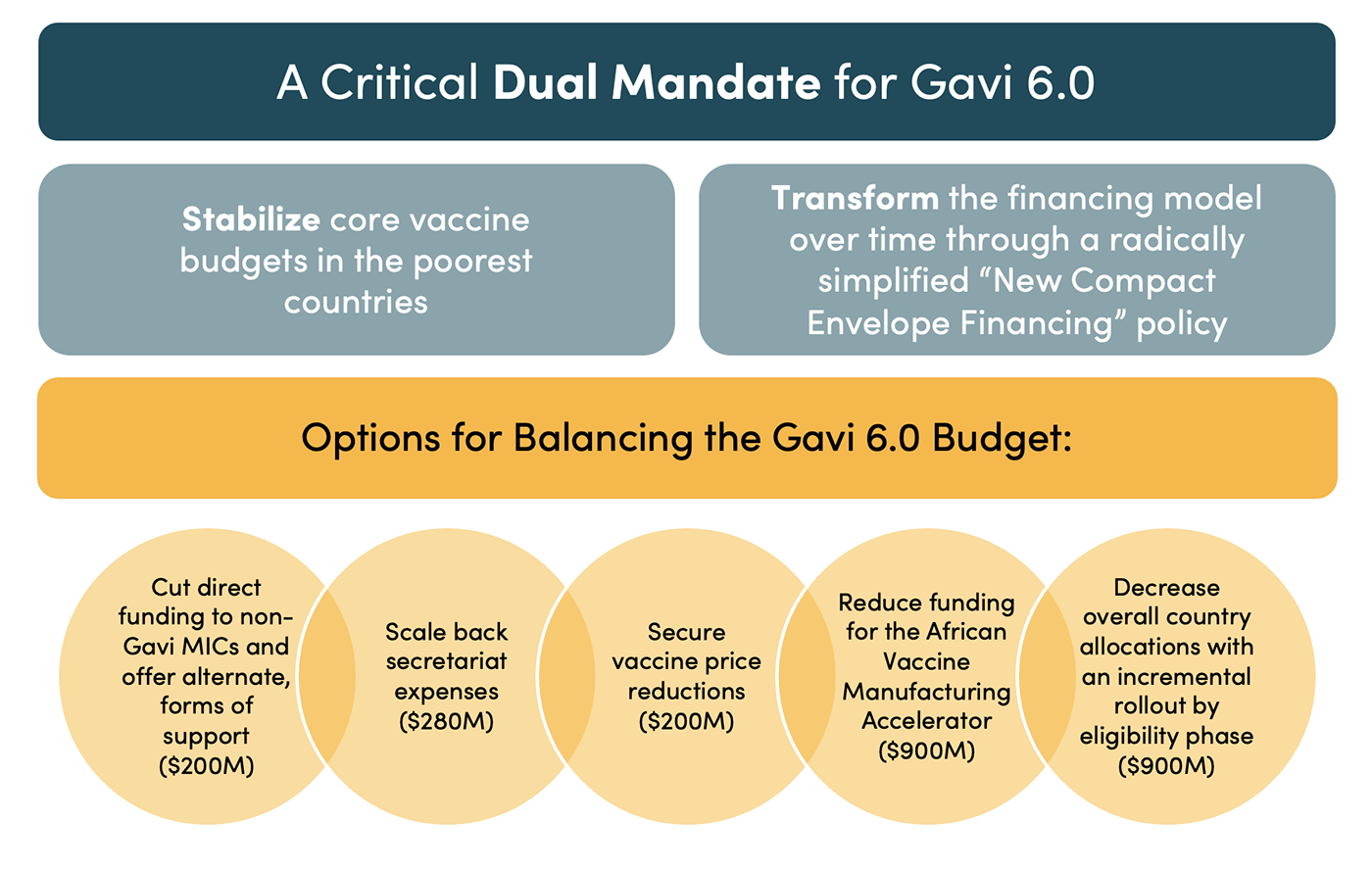
How Gavi 6.0 Can Take a Bigger Leap
The global health architecture is facing intense scrutiny. There are now an A-Z of initiatives launched to lead the reform, from the Accra Reset to the Lusaka Agenda Secretariat and a WHO-led process. Critics have argued that the current system fails to focus on the poorest countries, fragments national systems, undermines country ownership, and displaces domestic health spending. The shock to the system caused by US shifts in aid policy and cuts by other G7 nations has brought these challenges to the fore. But they are not new. The architecture was built by the G7 in the 2000s—and two decades later, it is increasingly clear it is not fit for a G20 world with rising non-communicable diseases (NCDs) and growing calls for health sovereignty.
Current reform processes have shied away from a precise prescription for a new financing mechanism. Without this there can be no progress. They have also neglected to fully consider the role of the multilateral development banks (MDBs). Over the past six months, researchers at CGD have been exploring the future role of MDBs in health. Here, I summarise one of our key recommendations: that an IDA Health Window—open to MDB cofinancing—has great potential to resolve the challenges of the current architecture. It could efficiently target scarce aid resources to the poorest countries and provide on-budget funding that respects calls for sovereignty whilst defragmenting financing and promoting impactful health systems. It could be delivered rapidly with minimal downsides, alongside IDA22 that will go into effect in mid-2028.
How would an IDA Health Window deliver on global health architecture reform?
An IDA Health Window at the World Bank would be a ringfenced pot for countries to seek finance for their health systems. It would be funded through IDA’s current system of replenishments, starting with IDA22 in 2028. Other donors and philanthropies that have specific interest in health could provide additional resources. It builds on IDA’s experience with a range of other windows and would be governed and operated through IDA’s usual processes. Let’s now see how an IDA Health Window could deliver on five key global health reform objectives:
Objective 1. Efficient targeting of limited grant aid to poorest countries
In an era of declining aid budgets, grants must be tightly focused. Resources should be stretched through the provision of concessional loans as countries develop, and a smooth transition between grants and loans is needed to avoid a financing cliff.
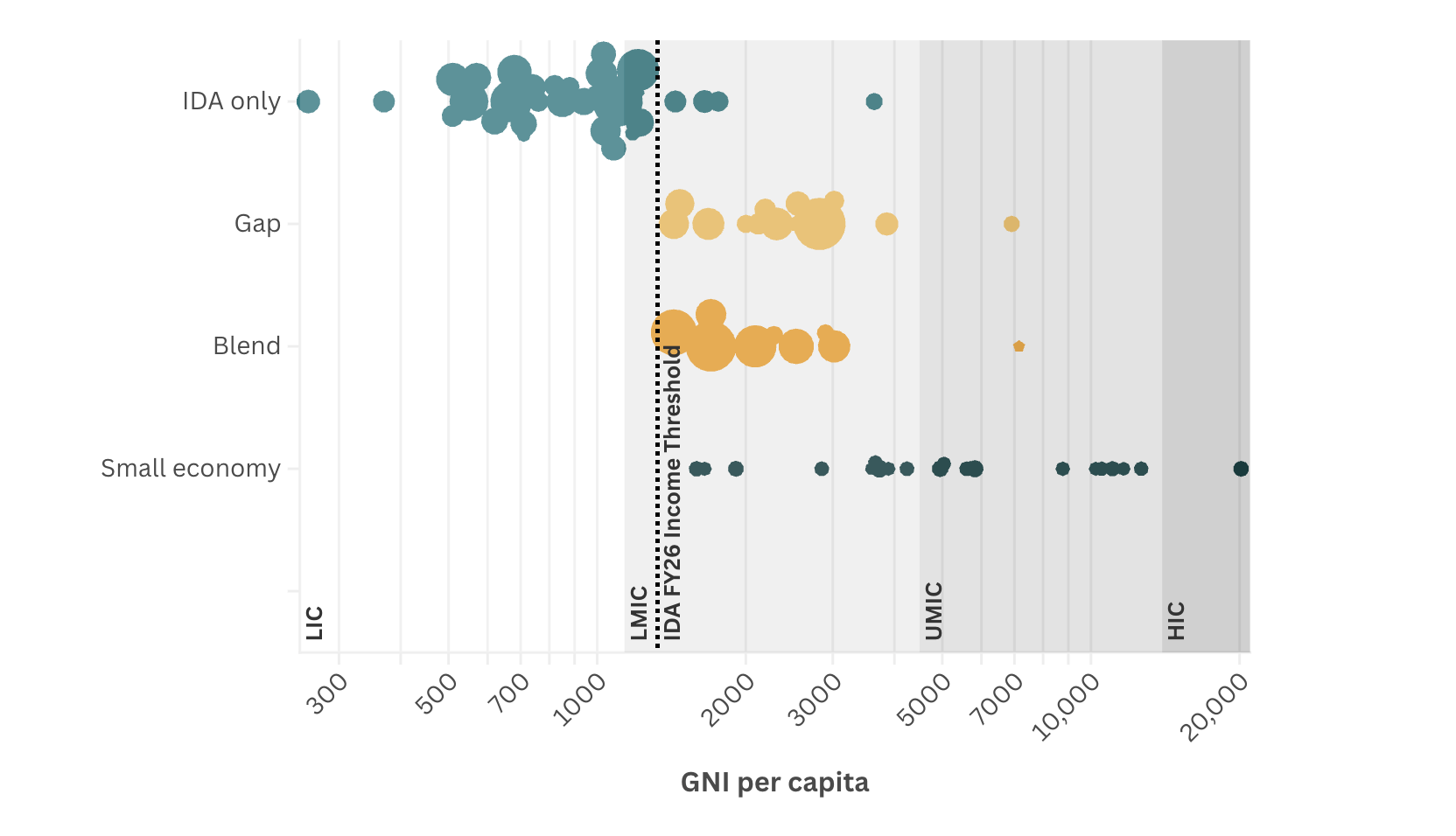
Eligibility for IDA is primarily determined by having a GNI per capita below $1,325, making it highly targeted to the poorest countries. We estimate that about 98 percent of IDA goes to low-income countries (LICs) and low- and middle-income countries (LMICs), and 75% of IDA allocations go to sub-Saharan Africa. The poorest and most vulnerable countries receive solely grant funding. But as countries get wealthier, they transition to concessional loans, and finally exit IDA support.
Objective 2. Maximise pooling of donor and domestic funds into a single budget
Consolidating donor funding, and pooling with domestic financing, reduces fragmentation and government administration costs. It also enables financing to be optimally allocated to a single combined set of priorities. Salaries, commodities, and capital can all be planned according to a single budget, with the objective of maximising the combined impact of pooled aid and domestic resources. This also creates incentives for donors and governments to invest in national systems and public financial management processes that are vital for long term impact.
IDA offers the potential to maximally consolidate donor financing into a single primary stream. It has much greater non-G7 sovereign funding than Gavi or Global Fund, offering the potential to channel wider G20 financing. It provides mostly on-budget financing, which enables domestic and aid financing to be pooled and allocated efficiently by treasuries.
Objective 3. Build health systems over time
Rising NCDs, alongside ongoing infectious disease burdens, and new breakthrough medical treatments have increased the complexity of health burdens that health systems must respond to. Twenty percent of HIV patients in sub-Saharan Africa have hypertension, for instance. A new financing mechanism must therefore support countries to develop broad platforms of health services and prevention.
IDA is disease-agnostic, on-budget, multiyear, and relatively stable between cycles, making it well placed to fund the development of health systems.
Objective 4. Respectful of health sovereignty
The Africa Centre’s for Disease Control and Prevention’s Africa's Health Security and Sovereignty Agenda and the Accra Reset are emblematic of a step change in demands for national control and financing of health systems. Health sovereignty may also enable achievement of the other objectives—increasing domestic financing, the building of systems, and maximising pooled impact of domestic and aid resources.
IDA grants and loans are on-budget and managed by governments in the main, therefore providing substantial sovereignty about how they are used. They do have conditions, however. And depending on the instrument disbursement may be dependent on governments achieving certain milestones.
Objective 5. Achieve ambitious but realistic reform
Reform must rapidly achieve its objectives while sustaining donor interest in financing. It must be feasible within the current and likely future financial, political, and technical contexts, with a realistic approach to both evolution and the end goal.
An IDA Health Window has the potential to transform global health financing. It would be a relatively simple change that would mostly use existing IDA processes. It would not substantially increase bureaucracy or require the complex transformation process of alternatives such as a Gavi and Global Fund merger. By offering a mechanism that earmarks resources for health, it may be able to maintain the interest of donors with a specific health interest.
Three risks to mitigate
The first key risk of an IDA Health Window is that the resources provided are not truly additional to health, and countries' existing IDA spend on health simply moves from core IDA to the new window. This could be mitigated by a matching arrangement, where a country’s IDA Health Window allocation is matched 1:1 with every dollar from their IDA allocation allocated to health.
A second risk is the difficulty of measuring impact. This could result in donors reducing funding. This could be mitigated by defining and tracking a set of core health system indicators, by mandatory health and healthcare surveys, by public expenditure reviews and impact evaluations (as was done by the Health Results Innovative Trust Fund), and by adding a performance tranche to the window—perhaps 30% of the total—which would only be released to countries that achieved progress.
A third risk is that resources are taken from Gavi and Global Fund. This would undermine their ability to deliver on their pooled procurement, technical assistance, and key population functions. In the medium term, the home of these ongoing functions needs to evolve. But in the short term, this risk could be managed through a stepped transition, where Gavi and Global Fund’s broad health system financing and technical assistance is the first to be transitioned to the IDA Health Window (and/or other World Bank Trust Funds). Pooled procurement and civil society support would initially remain at Gavi and Global Fund.
Three complementary reforms beyond the IDA Health Window
An IDA Health Window cannot, and should not, try to do everything. In the medium term, three complementary financing and procurement reforms would optimise its impact:
- A health commons trust fund should be established. This would cover areas with international externalities that countries are unlikely to use the IDA Health Window for, unless incentivised, such as pandemic preparedness and antimicrobial resistance. The Pandemic Fund could naturally evolve into this.
- Public development banks sit on $23 trillion of assets. Greater co-financing between IDA and other multilateral and national development banks could be impactful, supported by the Global Collaborative Co-Financing Platform.
- A new market-shaping and pooled procurement architecture is needed to ensure efficient use of window’s resources. With the diversifying of the disease burden faced by IDA-eligible countries, this must be for all health commodities, centrally facilitated and informed, but built from the bottom up by countries and regions. This is likely to result in a “multi-lane” architecture, with government choice of which to use with IDA resources.
Figure 1. Design of an IDA Health Window

A two-step implementation path
To implement the window, the World Bank should develop a detailed two-step proposal in 2026. Following approval by IDA deputies, the first step would establish the window, and donors would provide resources as part of the IDA22 replenishment negotiations in 2027. The IDA Health Window would then be launched in mid-2028. Gavi and the Global Fund boards would progressively transfer their substantial health system financing and technical assistance funding to the IDA Health Window and/or appropriate existing trust funds. They would “radically simplify” and focus on their procurement comparative advantage and key population support.
Step two would form part of IDA23 in 2031, with a full IDA Health Window, and completion of the complementary reforms, including a health commons trust fund and a new global market-shaping and pooled procurement architecture.
Figure 2. Two steps to an IDA Health Window

Conclusion
An IDA Health Window provides a clear vision for the future of global health financing. It can resolve many of the current challenges such as fragmentation, inefficiency, and lack of country ownership. It maximally pools donor resources, targets the poorest countries, and enables blending of grants and loans as countries develop. It respects health sovereignty, and through on budget funding, makes possible the efficient allocation to a single set of priorities and the building of strong health systems. It is fully aligned with the principles of the Accra Reset, African Union, and Africa CDC health financing policies. It can also be a short-term win, established at minimal cost, and with minimal harm to the current system, yet providing a scalable and natural pathway out of the current architecture.
With thanks to Rachel Bonnifield for co-developing the ideas in this blog, Clemence Landers for comments and advice, Rosie Eldridge for research support, and insights from members of a CGD private roundtable on this topic in February 2026. All errors are mine.
Topics
DISCLAIMER & PERMISSIONS
CGD's publications reflect the views of the authors, drawing on prior research and experience in their areas of expertise. CGD is a nonpartisan, independent organization and does not take institutional positions. You may use and disseminate CGD's publications under these conditions.
Thumbnail image by: Author