Recommended

BRIEF
A Radically Simplified Global Fund to Meet the Moment
BRIEF
How Gavi 6.0 Can Take a Bigger Leap
Summary
The global health architecture is facing a crisis of both financing and legitimacy. Gavi, the Vaccine Alliance and The Global Fund to Fight AIDS, Tuberculosis and Malaria have had their budgets cut by over 20 percent, donors are urgently calling for reform, and low- and middle-income nations are demanding greater sovereignty over their health systems. Current reform processes have shied away from a precise prescription for a new financing mechanism. Without this, there can be no progress. An International Development Association (IDA) Health Window would resolve the challenges of the current architecture. This brief outlines its mission, policy objectives, and key design characteristics. It builds off a forthcoming working paper which reviews the World Bank’s role in health financing.
An IDA Health Window would be a ring-fenced fund at the World Bank for countries to seek support for financing their health systems. It would have a single, clear mission: to drive down mortality in low- and middle-income countries through the expansion of basic, cost-effective health services. It would significantly contribute to the World Bank’s target of delivering health services to 1.5 billion people. It has five main benefits that distinguish it from the current global health architecture. First, it can draw in G20 donors beyond the G7, pooling their funding and defragmenting health financing. Second, it can better target aid to the poorest countries. Third, it can blend grants and loans to stretch resources further and enable a more sustainable transition from aid. Fourth, it can provide on-budget funding without earmarks, thereby building impactful health systems. Lastly, it can deliver on widespread calls for health sovereignty.
It is an ambitious proposal, but realistic if it is adopted by the World Bank in a two-phase approach. Phase 1—comprising $1.75 billion—could be delivered rapidly with minimal downsides alongside IDA22, which comes into effect in mid-2028. Given global aid cuts, phase 1 would not seek additional money, but instead would redirect health system strengthening financing into IDA. Phase 2 would see a $4 billion window launched as part of IDA23 in 2031. The IDA Health Window would then become the primary multilateral route for health aid, consolidating 33 percent of development assistance for health, and would be accompanied by a set of complementary global health reforms. This two-phase approach would enable it to be established at minimal cost and with minimal harm to the current system; with the second phase resulting in a scalable and seamless pathway out of the current architecture.
I. Introduction
The global health architecture is facing a crisis of financing and legitimacy. Two of the biggest heavyweights in the space, Gavi, the Vaccine Alliance and the Global Fund to Fight AIDS, Tuberculosis and Malaria, have had their budget cut by over 20 percent, donors are calling for reform, and low- and middle-income countries (LMICs) are demanding greater sovereignty over their health systems. Cuts to aid by the US, UK, and other G7 nations in 2025 have increased calls for reform. In response, several initiatives have been set up to guide reform, including the Accra Reset, the African High-Level Ministerial Committee on Global Health Architecture Reform, and a World Health Organization-led process. Three specific challenges in global health financing have been identified:
- Maldistribution. Low-income countries (LICs) are most in need of support and least able to finance their own health systems. Yet in 2023, they received only 37 percent of country-allocable development assistance for health (DAH).[i] With grant resources increasingly scarce, these need to focus more on LICs.
- Fragmentation. Countries receive multiple off-budget and earmarked (disease- or intervention-specific) grants from different partners. These grants are often uncoordinated, resulting in fragmentation of health systems. This fragmentation leads to a high management burden for low- and middle-income country (LMIC) governments, and undermines national planning and priority-setting, resulting in low allocative efficiency and displacement of domestic health spending.
- Built by the G7 for priorities of the 2000s. Gavi and the Global Fund were created in the 2000s, when the G7 held greater dominance, aid was increasing, and combatting infectious diseases was the overwhelming priority. Today, the G7 continues to provide over 90 percent of Gavi and Global Fund resources, but its share of global GDP is just 28 percent. Economic growth, ageing populations, and epidemiological progress against infectious diseases means non-communicable diseases will rise to more than 50 percent of the disease burden in all regions, including Africa, by 2030. A new financing mechanism must therefore attract wider G20 support, and enable LMICs to build broader health services that can respond to the diseases they now face.
So far, current reform processes have shied away from a precise prescription for a new financing mechanism that would respond to these challenges. This brief proposes a new solution: an IDA Health Window, a ring-fenced fund at the World Bank to finance health systems in LMICs.
Section II outlines the mission and objectives of the IDA Health Window, and whether it could respond to the three challenges set out above. Section III discusses the key characteristics of the IDA Health Window to optimise its impact and reduce its risks. Finally, section IV sets out a two-phase implementation approach and how it would be funded.
II. The mission and objectives of the IDA Health Window
Mission
The IDA Health Window’s mission would be to accelerate progress towards ending preventable deaths in the world’s poorest countries. It would achieve this by partnering with IDA countries to sustainably finance and maximise the delivery of essential, high-impact, cost-effective health services. This would enable more health workers to deliver effective maternal and newborn care, expand access to life-saving interventions against infectious diseases, and strengthen the delivery of essential health services. By focusing scarce concessional finance on essential services for the poorest countries, the IDA Health Window could become one of the world’s most effective financing instruments for reducing child mortality while representing a step change in the World Bank’s ambition to expand access to healthcare for 1.5 billion people by 2030.
An IDA Health Window should deliver on five key objectives (Figure 1):
Figure 1. Five objectives of an IDA Health Window

Objective 1. Maximise pooling of G20 donor funds
Consolidating donor funding, and pooling with domestic financing, reduces fragmentation and government administration costs. It also enables financing to be optimally allocated to a single combined set of priorities. Salaries, commodities, and capital can all be planned according to a single budget, with the objective of maximising the combined impact of pooled aid and domestic resources. This also creates incentives for donors and governments to invest in national systems and public financial management processes that are vital for long-term impact.
IDA offers the potential to maximally consolidate donor financing into a single primary stream. Like Gavi and the Global Fund, it can consolidate G7 donor funding. But it can go much further because other G20 nations provide 34 percent of its funding. Indeed, China is IDA’s fifth biggest contributor.
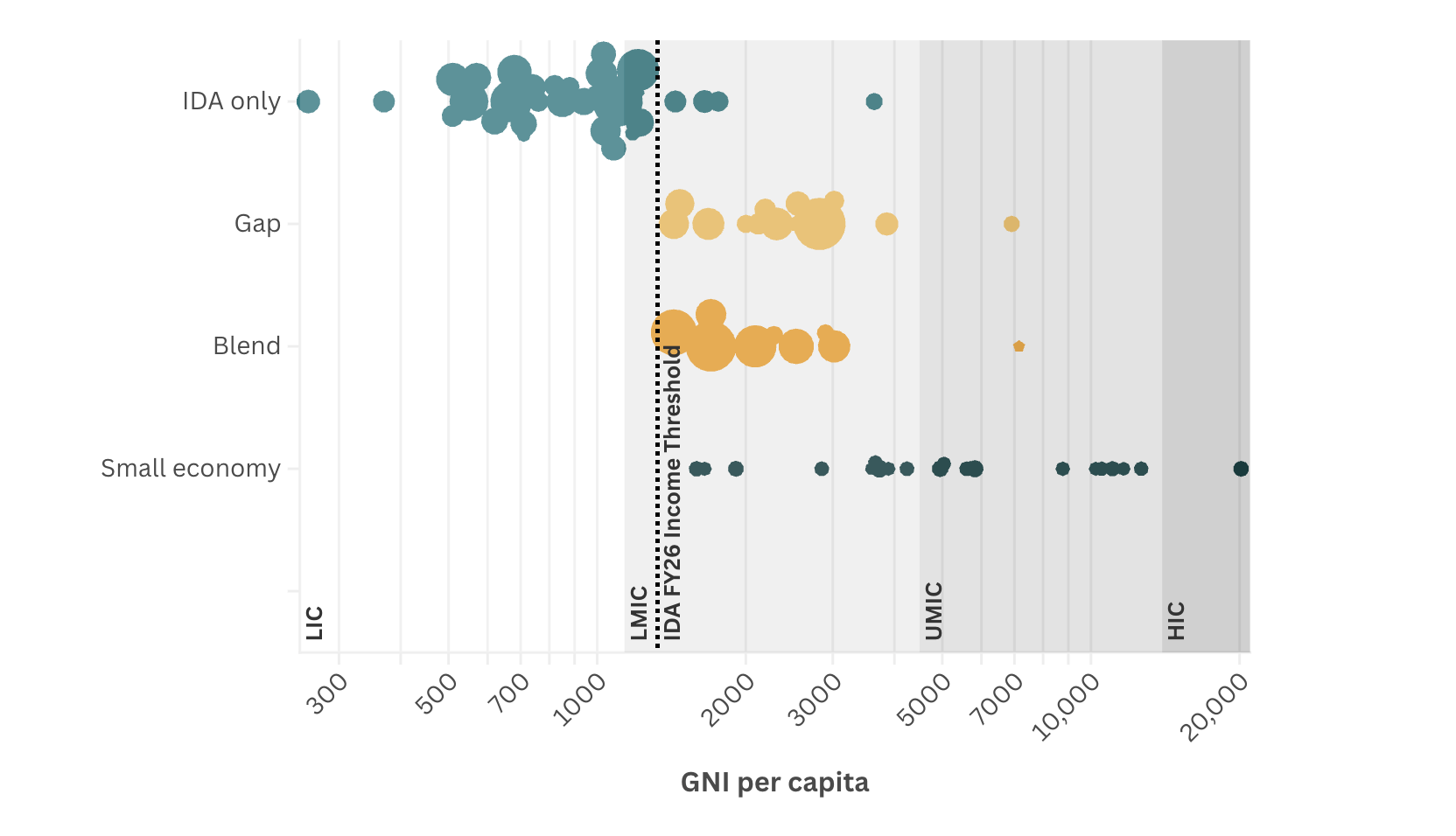
Objective 2. Focus aid on low-income countries
In an era of declining aid budgets, grants must focus on the poorest countries. IDA is focused on LICs because eligibility is primarily determined by a GNI per capita income threshold of $1,325, although it does provide support to countries above this for a transition period. Indeed, a forthcoming CGD paper finds that 49 percent of IDA health grants and loans go to LICs—a substantial improvement on DAH’s 37 percent allocation to LICs.
Objective 3. Use loans to stretch aid further and for sustainable aid transition
IDA provides grants for the poorest and most economically vulnerable countries and concessional loans to countries as they get richer. Concessional loans produce reflows and can be supported by private capital borrowing, which means IDA can provide much more support than if it was solely a grant-making institution. Reflows and private borrowing make up three out of every four dollars IDA provides.
Transitioning wealthier countries away from aid has been challenging for both Gavi and the Global Fund, which have found that countries have become dependent on their support. Loans provide IDA with an additional stepping stone to sustainable domestic financing that exclusively grant-based models cannot do. This is an important step in the transition process because loans are less likely to displace domestic financing.
Objective 4. Provide on-budget financing for a basic package of essential services
Rising non-communicable diseases, alongside ongoing infectious disease burdens, and new breakthrough medical treatments have made health burdens more complex for health systems to manage. Twenty percent of HIV patients in sub-Saharan Africa have hypertension, for instance, resulting in the same patients needing treatment for both illnesses. Responding efficiently requires broad platforms of care (e.g., delivered by community health workers) that can deliver basic, highly cost-effective services to all regardless of disease. This means shifting from a single disease focus to building system capabilities, such as planning and priority-setting, service coverage, supply chains, and data systems.
IDA is disease-agnostic, on-budget, multiyear, and relatively stable between cycles, making it well placed to fund broad development of health systems. By partnering with ministries of finance and using public financial management systems, it also builds country capacity to use domestic resources in the long term. Its multisectoral nature also enables it to fund projects on wider population health, disease prevention, and the social determinants of health which could increase the return on investment.
However, the Bank is not a health agency. To effectively scale up its health work, it will need to collaborate better with other expert agencies, particularly the World Health Organization. It will also need to cultivate and fund an ecosystem of technical assistance providers to support countries in the design and execution of its programmes.
Objective 5. Respect health sovereignty
The Africa Centres for Disease Control and Prevention’s Africa's Health Security and Sovereignty Agenda and the Accra Reset both mark a step change in demands for national control and financing of health systems. Calls for greater health sovereignty stem from democratic principles, but in addition, if governments are seen by citizens to be fully accountable for their health system, they may, in turn, increase domestic financing.
At an operational level, IDA grants and loans are substantially more aligned with country sovereignty. The vast majority are on-budget and managed by governments, providing substantial country control. But they do have conditions. Depending on the instrument used, disbursements may be dependent on governments achieving certain milestones, agreed with the World Bank. Country control is also in tension with the World Bank’s governance framework, which provides greater votes for major donor country shareholders. However, the same is also true of Gavi and the Global Fund. Specifically, IDA-eligible countries have 15.2 percent of votes on the Board, compared to Gavi’s 18.5 percent and Global Fund’s 35 percent of Board seats allocated to implementing countries.
Overall, an IDA Health Window would provide slightly less LMIC input into Board-level decisions than Gavi and the Global Fund, in return for greater country sovereignty over how the money is used.
Is an IDA Health Window politically and technically feasible?
If the above objectives are met, an IDA Health Window would be attractive to both donor and recipient countries. And administratively, it is remarkably feasible. It could be launched as part of IDA22 in 2028, and it would not substantially increase bureaucracy or require the complex transformation process of alternatives such as a Gavi-Global Fund merger. There are risks, however, and there are stakeholders who will resist change. Therefore, Section III looks at the optimal design of the window, how to mitigate known risks, and increase stakeholder support for the proposal.
III. Optimal design of an IDA Health Window
How does IDA currently fund health?
IDA is already a major source of health system financing, spending approximately $3.5 billion a year. It is funded primarily (75 percent) by reflows from historic loans and market borrowing, plus a donor replenishment every three years which makes up the remaining 25 percent. It allocates resources to countries through a formula based on GNI per capita and an assessment of economic policies and vulnerability. Depending on a country’s vulnerability, the allocations may be provided as grants (24 percent) or concessional loans (76 percent). IDA is not earmarked and countries may choose how much of it is spent on health. A forthcoming CGD paper finds that 90 percent of IDA-eligible countries choose to have an IDA health operation, and the median country allocates 7 percent to health. These resources are important for country health systems—at the median, they provide the equivalent of about 17 percent of government health expenditure.
On top of their core allocation, countries can request additional resources through specific trust funds, such as the Global Financing Facility for Women, Children and Adolescents (GFF) and IDA “windows.” These windows are earmarked pots for specific policy areas like regional challenges, private sector investments, or response to crises.
How would an IDA Health Window differ from IDA’s current approach?
The primary difference is that an IDA Health Window would be earmarked for health. Therefore, it can attract donors to IDA who want to guarantee that their resources will be directed to health. It would be funded through IDA’s current system of replenishments, starting with IDA22 in 2028. Donors would pledge a specific amount to the window during this replenishment. Additional donors with a health interest, but who currently do not contribute to IDA, could add extra funds. It would be a relatively simple change that would be governed and operated using existing IDA processes. Allocation to countries would follow the same formula as the current performance-based allocation IDA process. Health Window-funded operations would be IDA operations, designed with countries in the same manner as all IDA operations and approved by the IDA Executive Directors.
An IDA Health Window would differ substantially from current trust funds—specifically the GFF. First, the GFF is relatively small, providing $147 million in 2025, only 4 percent of IDA’s health financing contribution. Second, as it is a trust fund, it can only provide grants and cannot benefit from the advantages of loans. Third, its administration is separate and additional to IDA—in other words, it has a separate investment case process, and a Trust Fund Committee controlled by a few donors. Fourth, the GFF has a defined scope within heath and cannot cover all health areas. An IDA Health Window would ideally be large ($1.75 billion), provide grants and loans, and be administratively simpler by following core IDA governance and rules.
Design elements to mitigate four key risks
Risk #1: The IDA Health Window “splits the IDA pot,” preventing countries from choosing how much to allocate to each sector. This outcome is likely if donors pledge less to core IDA and shift their money to the IDA Health Window. This is a broad and legitimate objection applied to all newly proposed windows, and it could prevent a viable political coalition forming around the IDA Health Window, with resistance from ministries of finance in both donor and recipient nations. However, the case for a Health Window is clear from the large volume of global health financing—over $30 billion a year—that is currently not in IDA, and which is highly earmarked by donors, contributing to the fragmentation of health systems. This in turn is driven by donors having a particular interest in health and specific requirements about how funding is spent and what impact it should have. This need cannot fully be met within current IDA processes.
Solution: IDA deputies in the next replenishment should agree that the purpose of the Health Window is to bring additional money into IDA from other sources, and thereby improve multilateral financing of health, whilst maintaining the core IDA fund levels. This additionality could be implemented with a rule that donors would only be able to contribute to the IDA22 Health Window if their core IDA22 pledges match or exceed their previous core IDA21 contributions.
Risk #2: Resources provided to the IDA Health Window are not additional to health, and countries’ existing IDA spend on health simply moves from core IDA to the new window.
Solution: Implement a matching arrangement, where a country’s IDA Health Window allocation must be matched 1:2 with their core IDA allocation. For example, if a country sought $25 million from the IDA Health Window, it would need to show how it was using $50 million of its core IDA allocation for health. The IDA20 Regional Window used a similar matching system.
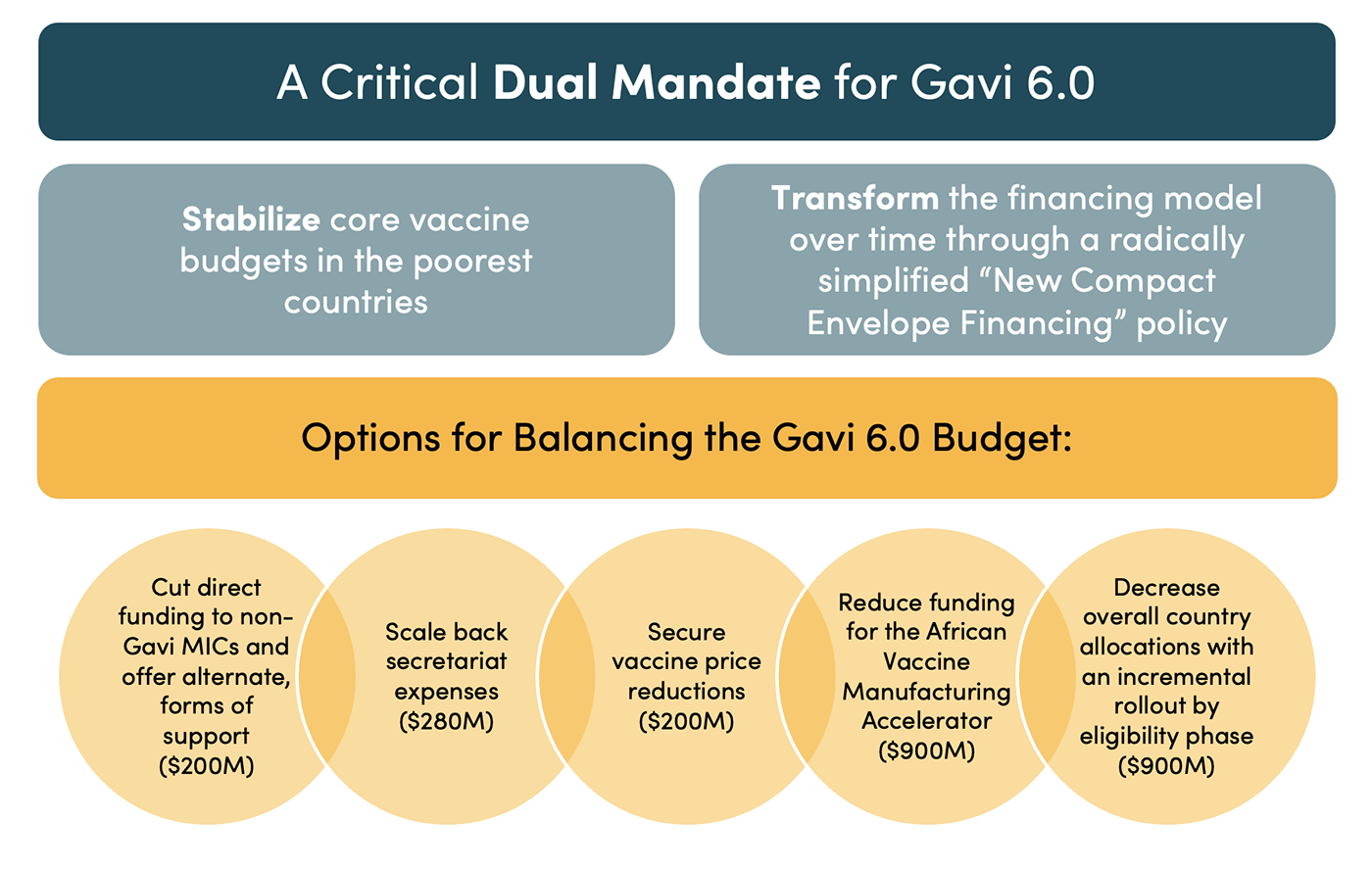
Risk #3: An IDA Health Window reduces resources for Gavi and the Global Fund, undermining their ability to deliver on their current pooled procurement and key population support functions. This risk could also lead to considerable opposition to the IDA Health Window, making it politically impossible.
Solution: In the short term, this risk could be managed through a two-phase transition. Gavi and the Global Fund’s broad health system financing and technical assistance functions would be the first to transition to the IDA Health Window, including a small (5 percent) earmarking for country-managed technical assistance. Pooled procurement targeted off-budget services for key and neglected populations, and civil society support would initially remain at Gavi and the Global Fund. This would allow these agencies to refocus on these core functions and could reduce political resistance to the IDA Health Window proposal. In the medium term however, it is widely recognised, including by Gavi itself, that these institutions need to be time limited due to changing burdens of disease, sustainability, and health sovereignty. An IDA Health Window is well placed to take over from them.
Risk #4: Measuring and modelling impact would be difficult, which could result in donors reducing funding.
Solution: For the IDA Health Window to succeed, it must get better at measuring impact and telling a strong narrative of the value of the investment. This could be done by defining and tracking a set of core health system indicators, by mandatory health and healthcare surveys, by public expenditure reviews and impact evaluations (as was done by the Health Results Innovation Trust Fund), and by a concerted effort to model impact and report these findings to donors and civil society. There could also be a performance tranche added to the window—perhaps 30 percent of the total—which would only be released to countries that achieved progress. The World Bank has a range of tools for this, and 25 percent of health commitments flow through Program-for-Results instruments that pay out on delivery of targets.
Four complementary reforms beyond the IDA Health Window
An IDA Health Window cannot, and should not, try to do everything. In the medium term, four complementary financing and procurement reforms would optimise its impact:
- Country coordination platforms should be established by all countries, and all multilateral and bilateral health funders should adopt a policy to join these where present, and pool funding collectively, where possible. This would enable the Bank and governments to ensure the IDA Health Window is used efficiently and is harmonised with other more earmarked funding. It would also present an opportunity for increasing civil society engagement. This could be an evolution of the Bank-supported National Health Compacts.
- Co-financing with wider public development banks and regional development banks should be the norm. Public development banks sit on $23 trillion of assets. Regional development banks, particularly in Asia and Latin America, have substantial resources and experience in strengthening systems in their regions. Thus, greater co-financing between IDA and other multilateral and national development banks could be impactful and encouraged through simplifying and aligning processes for co-financing, supported by the Global Collaborative Co-Financing Platform.
- A Health Commons Trust Fund should be established. This would cover areas with international externalities that countries are unlikely to use the IDA Health Window for, unless incentivised, such as pandemic preparedness and antimicrobial resistance. The Pandemic Fund could naturally evolve into this.
- A comprehensive, country-led pooled procurement architecture is needed to ensure efficient use of the window’s resources. With the growing disease burden faced by IDA-eligible countries, this must cover all diseases and technology areas, be centrally facilitated and informed, and country-led, built from the bottom-up by countries and regions. This is likely to result in a “multi-lane” architecture, with government choice of which to use with IDA resources.
Figure 2 summarises the window’s proposed design. Fundamentally, it should be kept simple and as close to IDA processes as possible, yet it should also include mitigations for the four key risks. Including the four complementary reforms would make the window even more successful. Section IV now sets out exactly how the window could be implemented.
Figure 2. Design of an IDA Health Window

IV. A two-phase implementation path
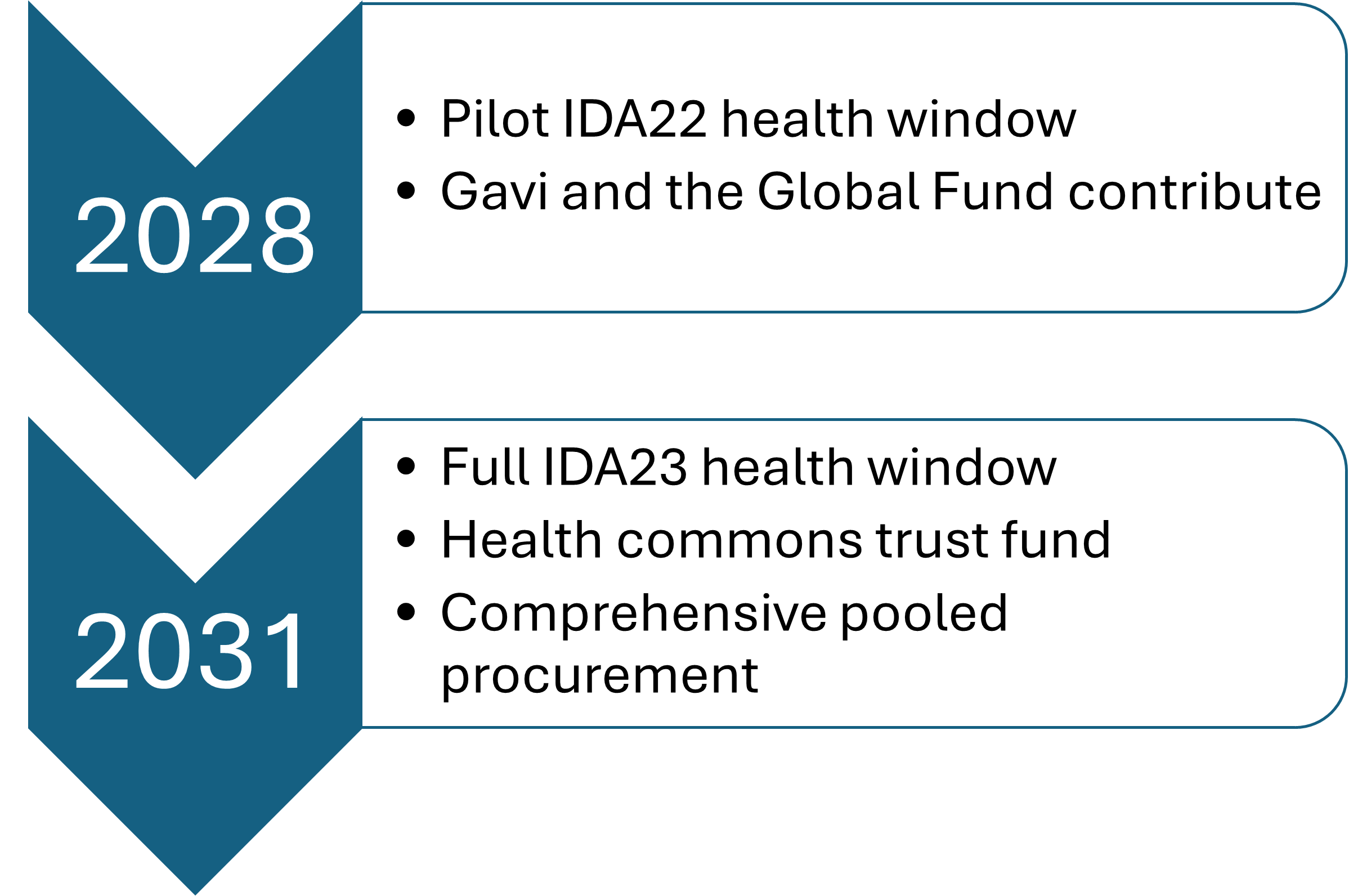
To implement the window, the World Bank should develop a two-phase proposal (Figure 3). Following approval by IDA deputies, the first phase would involve establishing the window, and donors would provide resources as part of the IDA22 replenishment negotiations in 2027, showing how contributions to the IDA Health Window are additional to their core IDA pledges. The window would then be launched in mid-2028.
To avoid taking resources from other sectors, the core IDA contribution to health should stay at its current figure of $3.5 billion. With 1:2 matching, this means the IDA22 Health Window in 2028 could be $1.75 billion annually. Thus, total IDA spend on health would rise from $3.5 billion to $5.25 billion a year without harming other sectors. The additional $1.75 billion for the window could be comprised of $1.25 billion a year redirected by donors from Gavi and the Global Fund’s health system strengthening budgets, and $0.5 billion from existing G7 nation bilateral health programme budgets. Gavi and the Global Fund would “radically simplify” and focus on their procurement comparative advantage and key population support.
Phase 2 would form part of IDA23 in 2031, with a full IDA Health Window and completion of the complementary reforms, including country platforms, co-financing arrangements with other multilateral development banks, a Health Commons Trust Fund, and a comprehensive global market-shaping and pooled procurement architecture. This step would be more ambitious, with the objective of consolidating the majority of multilateral spend into IDA and an aggregate increase in total DAH. As an example scenario, the window could be $4 billion a year, inclusive of winding down funding to Gavi, the Global Fund, and other global health initiatives, and shifting resources to IDA, including wider G20 bilateral health aid. If this was matched 1:2 with IDA health spend, it would result in total IDA funding of $12 billion a year—approximately 33 percent of all DAH.
Figure 3. A two-phase approach to implementing an IDA Health Window

V. Conclusion
An IDA Health Window provides a clear vision for the future of global health financing. If political will can be mobilised then the potential payback is large. An IDA Health Window can bring in new G20 donors and pool their resources, defragmenting health financing; it can offer better targeting of the poorest countries; and blend grants and loans to stretch resources further. It respects health sovereignty, and through on budget funding, makes possible the efficient allocation to a single set of priorities and the building of strong health systems. It is fully aligned with the principles of the Accra Reset, the African Union, and the Africa Centres for Disease Control and Prevention’s health financing policies. By bringing in resources from G20 bilateral health spend, Gavi, and the Global Fund, it can avoid taking resources from other sectors and minimise the harm of fragmenting the IDA pot. It can deliver quick results in phase 1, set up with minimal cost, and with minimal harm to the current system, yet provide a scalable and seamless pathway out of the current architecture. It will become the Bank’s primary route to achieving its target of delivering health to 1.5 billion people, as well as the world’s primary multilateral financing mechanism to drive down mortality in LMICs.
Thanks to Rachel Bonnifield and Clemence Landers for comments and advice in the development of the ideas in this brief, Rosie Eldridge for research support, and insights from members of a CGD private roundtable on this topic in February 2026.
[i] Based on authors’ calculations using IHME’s Development Assistance for Health Database (1990–2025) (https://ghdx.healthdata.org/record/ihme-data/dah-1990-2025-20251114)
Topics
CITATION
Baker, Pete. 2026. An IDA Health Window: The Future of Global Health Financing. Center for Global Development.DISCLAIMER & PERMISSIONS
CGD's publications reflect the views of the authors, drawing on prior research and experience in their areas of expertise. CGD is a nonpartisan, independent organization and does not take institutional positions. You may use and disseminate CGD's publications under these conditions.