Recommended


CGD NOTE
The Evolution of Health Benefits Packages in Colombia

Event
Celebrating a Decade of Health Prioritization
VIRTUAL
July 09, 2024 10:00—11:00 AM EST | 3:00-4:00 PM BSTThis note is the introduction to a special issue of Health Systems & Reform, "Building Institutions for Priority-Setting in Health" edited by Victoria Fan and Javier Guzman, with Pete Baker. Read the article introducing the issue, online here. The special issue covers priority-setting institutions that serve 50 percent of the world's population, including two of the world's largest countries, with 20 articles and over 75 authors from more than 15 countries.
In the pursuit of universal health coverage, countries are invariably confronted with questions about which services to pay with public funds, to whom, and at what cost. Such priority setting processes have major ramifications for the costs and benefit of care delivered. These processes are not just technical, but also highly political and organizational in nature and expressions of social values. This special issue focuses on building institutions for priority setting in health. These institutions serve a public purpose and are primarily concerned with conducting or using health technology assessment (HTA) to inform resource allocation decisions.
Organizations, agencies, and institutions are terms used in this introduction in the following ways. An organization is the most general classification, inclusive of agencies and institutions, and refers to a “formal, goal-orientated group with members and a defined structure, governed by rules and procedures that guide operation.”1An agency refers to a government organization, or an organization that provides a specific service, whereas a “public agency” is codified in various US laws in general reference to a federal, state, or substate agency.2,3 Definitions of institution vary and are not universally accepted. We propose that the definition of institution has the twofold characteristics of durability and addressing (or being perceived as addressing) social needs.4,5,6 One definition of institution represents a public agency of lasting and enduring importance over time, with a “pursuit of aims that are widely considered to fulfil a societal need, its reliable performance over time, and its exemplary conduct as perceived by societal constituencies” or an organization that has “developed a consistent and effective way of working, which is strongly valued by internal and external stakeholders.”4 In the special issue, authors use these terms in different ways, sometimes interchangeably, and we do not constrain definitions across articles. In some circles, for example, these organizations are collectively self-referred to as “HTA agencies” as reflected in the International Network of Agencies for Health Technology Assessment, itself an organization of “HTA agencies.”7
Regardless of formal definitions, the term “institution” has an aura of being grander—such as being more durable and with a specific purpose—than an agency or an organization that can be created (or destroyed) by a change in government administration. An aspirational state for an organization, however, is important because an “institution” represents an ambitious goal. Thus, we have deliberately chosen as the title of this special issue “Building Institutions for Priority Setting” to recognize this aspirational state of an institution towards which organizations and agency can become. We are living in an era when many institutions, including key institutions of democracy in many countries, are being tested for their durability and perceived ability to serve social needs. So too do the articles in this special issue reflect various challenges and tests in these characteristics. Articles explain, and in some cases wrestle with, how priority setting and health technology assessment became a key purpose of an organization or agency and how those organizations emerge, are built, and evolve into institutions. Articles also reveal the interorganizational relationships—that is, between HTA institutions and their broader organizational ecosystem, including political and state institutions (e.g. the courts, legislature), ministries of health and finance, and academic institutions. Compared to these older institutions, the organizations described in this special issue have been in existence for at most a few decades, and in most cases far less than that or even organizations which have not yet been established. Thus, many countries are still in the early days of building institutions for priority setting for health.
In this introduction, we first define the concept of institutions for priority setting in health and the methodological considerations of assessing and evaluating these institutions. Next, we present key themes common and summarize key messages across the articles, including lessons learned and future challenges in building these institutions. We hope that these lessons may be relevant for other countries pursuing universal health coverage with priority setting.
Defining institutions for priority setting in health
This special issue presents 11 accounts of domestic experiences of building national institutions for priority setting in health.8–18 It also presents articles from organizations or networks engaged in supporting countries to create and strengthen these institutions, such as the International Decision Support Initiative (iDSI), a network created in 2013 to expedite HTA institutionalization in Asia and Africa.19–24 For the country cases, this special issue includes organizations conducting or using HTA to inform resource allocation decisions with the tools of comparative effectiveness, cost-effectiveness, and budget impact analysis. Excluded are organizations which use HTA as a secondary concern, such as the entire ministry of health which has a broader mandate. For articles that are not focused on specific countries, this special issue includes a piece on successes, challenges and lessons learned from iDSI,19 an article by Norheim and Watkins of the Disease Control Priorities Project that distinguishes between HTA and Health Benefits Packages (HPB),20 an article on priority setting in health using modeling methods at the World Bank,21 a literature review on the institutionalization of HTA across countries,22 a commentary on HTA process from the Norwegian Institute of Public Health,23 and an article examining HTA across Latin American countries through a network supported by the Interamerican Development Bank.24
How to evaluate institutions for priority setting in health
While institutions for priority setting in health conduct and use extensive evaluations and analyses of health interventions, there is not a globally agreed framework to evaluate what they do and how they do it using quantitative methodologies, and in fact evaluations are rarely done.25 Thus, their evaluation and assessment require the application of qualitative research methodologies, including archival and documentation research, historical analysis, and thematic analysis, among others. Chronology, that is, historical events over time, is the main variation used and examined in this special issue and often for a single country.
While such single-country cases are limited in their generalizability,26 this special issue as a whole seeks to mitigate this limitation by collectively representing nearly 50% of the world’s population, includes two of the world’s largest countries (India11,12 and China14) with 20 articles and over 75 authors from more than 15 countries.
Articles in this special issue also benefit from the roles of the authors in policy and practice: the authors of this special issue have participated in, worked for, established, or modified organizations. Many articles draw on the lived and deep experiences of authors in creating and building these institutions. They come from different backgrounds including government, international, civil society, and academia, or a combination thereof.
For this special issue, we selected articles presenting the historical growth of institutions for priority setting in health rather than evaluations of their impact or effectiveness per se. The article by Prinja and colleagues is the only article in this special issue that attempts to quantify the cost-effectiveness of doing cost-effectiveness analysis. This paper is emblematic of what an evaluation might require, by shedding light on the potential savings and efficiency gains of specific policy decisions that were made.12 The literature provides some estimates of the return of investment of using HTA in priority setting, estimating an eight- and nine-fold return on investment in Thailand and India respectively.27,28 These estimates align with the scoping review of institutionalizing HTA which postulated that the benefits outweigh the costs.22
Cross-country themes on building institutions for priority setting in health
In this introduction, we focus on what we consider to be the three most important themes that help to explain how to build these institutions and are shared among multiple cases: (1) the motivations for agenda setting and policy reform; (2) the importance of coalition building and capacity building and the role of citizens and the public; and (3) the specific organizational characteristics of different arrangements of institutions for priority setting in health.
Motivations for agenda setting and policy reform
The eleven domestic cases demonstrated the importance of getting HTA onto national policy strategy documents, which served as a focal area for policy entrepreneurs to build momentum and gain political commitments, in both HTA activities and in some cases, in creating or growing institutions to conduct or use HTA.8–18 The demands for negotiating drug prices (or dealing with a budget constraint), or separately, the demands for increasing coverage of benefits were reflected in the 11 domestic cases presented in the special issue.8–18 But while these two motivations are closely related, they are distinct motivations for propelling policy reform. In some countries, such as Colombia, Ghana, and South Africa, HTA was clearly linked to defining the national medicines lists or expanding the benefit package for the national health insurance plan,8–10 while others such as Thailand and China emphasized the role of HTA for price negotiations.13,14
The two cases of Colombia and South Korea reveal the socially contentious challenge and trade-offs to expanding benefits over limiting benefits to control the budget and/or maximize efficiency.8,16 These two cases also revealed the importance of public demand through social movements and citizen discontent and the critical ways in which state institutions (e.g., the courts, the president) responded to such public demand, outside the remit or circumventing decisions informed by HTA evidence. Notably, these cases emphasized the need for robust, participatory and transparent processes but also the tension between efficiency and concerns of equity and fairness and the role of public demand and social movements in calling for greater benefits but not in calling for greater efficiency.
Coalition building, capacity building, and public engagement
Coalition building across multiple organizations including academic institutions, government agencies, and the public was another common theme across all the country cases,8–18 although cases varied in the leadership and composition of those coalitions. Coalitions in Thailand, India, and Taiwan, for example, described in this issue emphasized the role of experts and technocrats.11,13,16 India, for example, drew on a wide network and coalition of partners across government, academic institutions, and healthcare providers, with arguably a less obvious role of civil society organizations in influencing the use of HTA or the creation of an HTA agency.11 In contrast, the case of South Korea and Colombia emphasized the importance of the public as a key stakeholder combined with political leadership.8,16
Building coalitions can involve the activity of capacity building, as shown in the cases of Thailand, India, and Taiwan.11,13,17 While coalition building and capacity building appear different in their purpose, in practice they are not easily differentiated because building a coalition around priority setting and HTA often requires training in how to interpret, use, and conduct HTA. HTA itself requires highly specialized training, revealing the importance of universities as well as nonformal training in order to build local capacity to conduct and use HTAs.11,13,17 These training arrangements were varied, including the learning-by-doing approach, international exposure and partnership such as by iDSI19 and others.
While expert specialization is commonly perceived as a strength of HTA, this specialization may also represent a political risk. In the case of South Korea, the most recent HTA institution that was developed had an explicit exclusion of experts; this suggests that experts may not be necessary to determine generosity of benefit packages and that their absence can be a politically expedient decision.16 In contrast, Teerawattananon and colleagues argue that greater public education of HTA is necessary for greater uptake and adoption of HTA.13 In South Korea, the provision of significant authority to the public to manage HTA processes and designing benefit packages can be added to the information prepared by HTA experts.16
Organizational design
The cases in this special issue reveal a variety of characteristics of how organizations are designed, even within the same country, particularly regarding where HTA assessments are conducted and their connection with policy decisions and decision makers. There is no common pattern that emerges among countries with multiple organizational designs, making it clear that there are many ways to organize different HTA activities and functions. Several countries created small technical units within the institutions that will use the HTA evidence (Ghana,9 and South Africa10 have units within the Ministry of Health, India has an agency within the Ministry of Health,11 and a unit within the national insurer,12 while South Korea has a unit within the national insurer16). Others created agencies separate from the decision makers but with close linkages through governance or financing mechanisms (Colombia,8 Indonesia,15 Thailand,13 Taiwan17,18 and South Korea,16 all have separate agencies informing the Ministry of Health, the national insurer or both). On the contrary, China has not created a permanent structure but rather convenes experts from academic institutions to conduct assessments, which then inform the national insurer.14
The country cases also reveal the diversity of features to consider when designing an organization, including the scope of activities (e.g., what type of study is conducted, what type of product prioritized), the degree of autonomy and public engagement (e.g., to what extent institutions conduct studies and make decisions based on evidence and public engagement), authority (e.g., to what extent does the institution have power to enforce or effectuate rules pertaining to HTA policy), financing (e.g., whether institutions are sustainably financed and have adequate human resources).
Autonomy as well as authority and policy relevance are major design features of these organizations that can be at odds with each other, as suggested by the cases of Columbia and South Korea.8,16 Whether the HTA organization itself has the authority to effectuate a policy decision (authority) is distinct from whether the same organization also has the independence to make those decisions without interference based on a political reason (autonomy). Having the autonomy to conduct independent, evidence-based HTA studies and processes means that the organization is protected from political or other interference, but its recommendations or findings may not be authorized with power to effectuate policy decisions. Having the authority to make decisions for coverage or pricing does not necessarily require autonomous decisions or decisions based on HTA. Finding a means to ensure that decisions are authorized and autonomous is the “sweet spot”—perhaps best exemplified by the case in South Korea where the public authority to make an autonomous decision successfully aligned these two features in a single organization16 (HIRA) and separately, the publicly led committee (PPSC).16 A third way to organize HTA agencies is by product type, with the most common product being essential medicines.
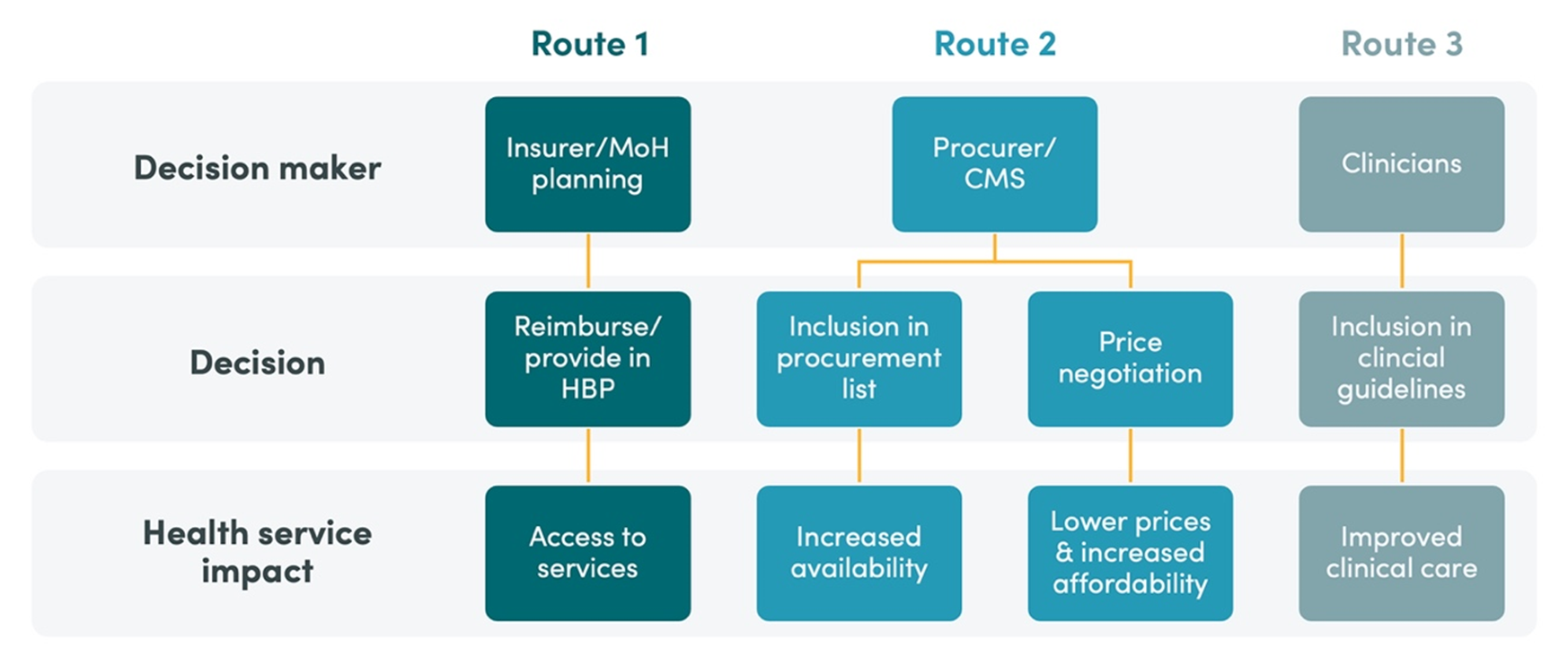
The variety of HTA activities can be divided up and assigned to multiple organizations. An HTA agency can adopt different HTA functions, based on activity (conducting studies or making policy decisions), methodology (effectiveness or cost-effectiveness) or product focus (medicines or technology or vaccines). Classification of these functions based on these categories is not mutually exclusive. Some countries have organized HTA by product and by activity (India11,12) or by product and by methodology (South Korea16). The division by activity, in which one organization conducts the HTA studies and another makes decisions based on the HTA processes, such as designing the HBP, determining prices and/or reimbursement rates, was observed in Colombia8, Thailand,13 Taiwan,17,18 South Korea,16 and India.12 A second way to organize HTA agencies is by type of study, shown by the agencies in South Korea that are organized in part by effectiveness (NECA) and cost-effectiveness (HIRA).
Shared challenges ahead
The institutions conducting or using HTA described in this special issue share many common challenges, including expanding the remit from medicines to other health technologies including public health interventions, timely reassessment of technologies, setting thresholds of what to cover and the challenges of the budget constraint, timely and prompt decision-making, stakeholder and public engagement, demonstrating value and impact of HTA studies, ensuring sustainability of an HTA agency along financial, human resources, and other operational dimensions, and using real world evidence and data.
Among these many challenges, the questions about the value and impact of HTA underpin several of these challenges and are crucial to the theme of building institutions—that is, the durability and the perceived public and social value. While typical HTA approaches in theory value stakeholder views, their ability to effectively address and meet the demands of the public is often questioned.8,13,16,17 Of all the cases, perhaps the example of South Korea reveals the most optimistic case of public support for evidence-based decisions due to public ownership and thus accountability.16 But in the absence of adequate public engagement, HTA can risk being used as a tool for justifying pre-determined benefit decisions based on cost and budget impact analysis.16,17
Conclusion
This special issue on “Building Priority Setting Institutions in Health” examines lessons from the developments and arrangements of different HTA agencies. This issue advances our understanding about the role of coalitions building, capacity building, and the public engagement, as well as the different functions and activities that HTA agencies adopt. It draws on both academic analyses and lived experiences and reflection of policy makers. The studies in this special issue are consistent with the literature on political economy for health policy about the importance about the role of agenda setting and coalition building.29–31 All the country cases reveal the intersection of public demand with political commitment in shaping policy agendas, coalitions being built, and organizations being established. Many of these organizations are new and young, with not more than 15 years of operations at best (Thailand) or 30 years of engagement (Colombia). The future of these organizations lies in their ability to become institutions that are durable (with adequate finances and human resources) and perceived social and public value (with broad consensus and agreement of the decisions made based on HTA). The work of agenda setting, coalition building, capacity building, and organizational implementation are areas that can be relevant for not only new students of public health but also policy entrepreneurs seeking to make new policy reforms in their bureaucracies. While policy entrepreneurs are crucial in these cases, perhaps the most important voices are those of the public who seek expanded benefit coverage in the face of budget constraints of national health programs.
References
- Bell K. organization. In: Open Education Sociology Dictionary. 2013. Accessed July 2, 2024. https://sociologydictionary.org/organization/
- Definition of agency. In: Cambridge Dictionary; 2024. Accessed July 2, 2024. https://dictionary.cambridge.org/us/dictionary/english/agency
- Public Agency. Vol 29 USC § 203(x). Accessed July 2, 2024. https://www.law.cornell.edu/definitions/uscode.php?width=840&height=800…
- Boin A, Fahy LA, ’t Hart P. Guardians of Public Value: How Public Organisations Become and Remain Institutions. (Boin A, Fahy LA, ’t Hart P, eds.). Springer Nature; 2021. doi:10.1007/978-3-030-51701-4
- Bell K. institution. In: Open Education Sociology Dictionary. 2013. Accessed July 2, 2024. https://sociologydictionary.org/institution/
- Rojas F. Institutions. In: Oxford Bibliographies. Oxford University Press; 2013. Accessed July 2, 2024. https://www.oxfordbibliographies.com/display/document/obo-9780199756384…
- The International Network of Agencies for Health Technology Assessment. INAHTA. Accessed July 2, 2024. https://www.inahta.org/
- Brun Vergara M, Garcia Ruiz J, Guzman J. The Evolution of Health Benefits Packages in Colombia: Thirty Years of Successes and Failures. Health Syst Reform. 2023;9(3):2343174. doi:10.1080/23288604.2024.2343174
- Koduah A, Anim Boadi J, Azeez JNK, et al. Institutionalizing Health Technology Assessment in Ghana: Enablers, Constraints, and Lessons. Health Syst Reform. 2023;9(3):2314519. doi:10.1080/23288604.2024.2314519
- Jugathpal J, Parrish A, Jamaloodien K, Blecher M, Daven J. Institutionalizing Health Technology Assessment in South Africa—An Opportunity in National Health Insurance. Health Syst Reform. 2023;9(3):2327098. doi:10.1080/23288604.2024.2327098
- Fan VY, Mehndiratta A, Ahazie J, et al. Organizational Formation for Priority Setting: Historical Perspectives and Thematic Analysis of India’s Health Technology Assessment Agency. Health Syst Reform. 2023;9(3):2327414. doi:10.1080/23288604.2024.2327414
- Prinja S, Chugh Y, Gupta N, Aggarwal V. Establishing a Health Technology Assessment Evidence Ecosystem in India’s Pradhan Mantri Jan Arogya Yojana. Health Syst Reform. 2023;9(3):2327097. doi:10.1080/23288604.2024.2327097
- Teerawattananon Y, Vishwanath Dabak S, Culyer A, Mills A, Kingkaew P, Isaranuwatchai W. Fifteen Lessons from Fifteen Years of the Health Intervention and Technology Assessment Program in Thailand. Health Syst Reform. 2023;9(3):2330974. doi:10.1080/23288604.2024.2330974
- Guo W, Wang P, Zhang Y, et al. Health Technology Assessment in China’s Health Care Sector: Development and Applications. Health Syst Reform. 2023;9(3):2327099. doi:10.1080/23288604.2024.2327099
- Wiweko B, Hidayat B, Nadjib M, Siti L. Moving from Traditional and Local HTA into Global and Standardized HTA Works: Platforms for HTA Bodies in Indonesia. Health Syst Reform. Published online 2024.
- Oh J, Kim MJ, Hur S, Oh J, Kim DS. Institutionalizing Health Technology Assessment and Priority Setting in South Korea’s Universal Health Coverage Journey. Health Syst Reform. 2023;9(3):2338308. doi:10.1080/23288604.2024.2338308
- Pwu RF, Cheng YS, Yang WW, Wu GHM. The Development of Health Technology Assessment in Taiwan: Perspectives and Analysis. Health Syst Reform. 2023;9(3):2330396. doi:10.1080/23288604.2024.2330396
- Chen SC. Health Technology Assessment in Taiwan: Reflections of the Last Twenty Years. Health Syst Reform. 2023;9(3):2330348. doi:10.1080/23288604.2024.2330348
- Baker P, Barasa E, Chalkidou K, et al. International Partnerships to Develop Evidence-informed Priority Setting Institutions: Ten Years of Experience from the International Decision Support Initiative (iDSI). Health Syst Reform. Published online 2024. doi:10.1080/23288604.2024.2330112
- Norheim OF, Watkins DA. The Role of HTA for Essential Health Benefit Package Design in Low or Middle-Income Countries. Health Syst Reform. 2023;9(3):2273051. doi:10.1080/23288604.2023.2273051
- Wilson D, Gorgens M. The Future of Priority Setting in Health in a Post-COVID World. Health Syst Reform. Published online 2024.
- Mbau R, Vassall A, Gilson L, Barasa E. Factors Influencing The Institutionalization of Health Technology Assessment: A Scoping Literature Review. Health Syst Reform. Published online 2024.
- Peacocke E, Heupink LF, Ananthakrishnan A, Frønsdal K. Is It The Right Topic? An Overlooked Stage In The Institutionalization of Health Technology Assessment. Health Syst Reform. Published online 2024. doi:10.1080/23288604.2024.2329082
- Giedion U, Espinoza MA, Gongor-Salazar P, Mehndiratta A, Ollendorff D. Harnessing Health Technology Assessment in Latin America and the Caribbean: A Long Journey Ahead to Tap Its Potential. Health Syst Reform. Published online 2024. doi:10.1080/23288604.2024.2314482
- Löblová O. What has health technology assessment ever done for us? J Health Serv Res Policy. 2018;23(2):134-136. doi:10.1177/1355819617725545
- Pepinsky TB. The Return of the Single-Country Study. Annu Rev Polit Sci. 2019;22(1):187-203. doi:10.1146/annurev-polisci-051017-113314
- Kingkaew P, Budtarad N, Khuntha S, et al. A model-based study to estimate the health and economic impact of health technology assessment in Thailand. Int J Technol Assess Health Care. 2022;38(1):e45. doi:10.1017/S0266462322000277
- Grieve E, Bahuguna P, Gulliver S, Mehndiratta A, Baker P, Guzman J. Estimating the Return on Investment of Health Technology Assessment India (HTAIn). Accessed April 30, 2024. https://www.cgdev.org/publication/estimating-return-investment-health-t…
- Reich MR. Political economy analysis for health. Bull World Health Organ. 2019;97(8):514. doi:10.2471/BLT.19.238311
- Reich MR. Applied political analysis for health policy reform. Curr Issues Public Health. 1996;2:186-191.
- Reich MR. Politics and Policies of Health Systems: Reflections on 50 Years of Observing Protests, Leaders, and Political Analysis. Health Syst Reform. 2023;9(1):2207296. doi:10.1080/23288604.2023.2207296
Topics
CITATION
Fan, Victoria, Javier Guzman, and Pete Baker. 2024. Building Institutions for Priority-Setting in Health . Center for Global Development.DISCLAIMER & PERMISSIONS
CGD's publications reflect the views of the authors, drawing on prior research and experience in their areas of expertise. CGD is a nonpartisan, independent organization and does not take institutional positions. You may use and disseminate CGD's publications under these conditions.



