Recommended

POLICY PAPER
A New Compact for Financing Health Services in Ethiopia

POLICY PAPER
Opportunities for Gavi and Partner Countries

Blog Post
The Global Political Economy of Health Financing Reform

CGD NOTE
Putting Aid in Its Place: Financing Common Goods
The Lusaka Agenda envisages fundamental shifts in the role of health aid towards sustainable domestically financed health services, country ownership, and donor alignment with country priorities and systems. In a previous policy paper CGD proposed a New Compact for health aid which is fully aligned with this vision. At the heart of the New Compact is the notion that existing power imbalances are redressed by countries setting a national package of health priorities and financing the core of this package, and donors align behind this by expanding what can be provided at the margin. Potential challenges with implementing the New Compact are not yet known, and so the aim of this note is to is explore the practical considerations for realising the New Compact in terms of public financial management (PFM), using the budget cycle—formulation, execution, monitoring—as a guiding framework. We find that the New Compact approach can support and promote the “one plan, one budget” vision, but need not be tied to a particular financing model such as direct budget support. The main PFM implications relate to budget formulation activities, although there are relevant considerations for execution and monitoring as well. The note goes on to explore PFM-related benefits and risks and argues that the New Compact is a promising concept whose implementation can be adaptable and pragmatic from a PFM perspective. While the approach holds potential for contributing to strengthening PFM systems, its implementation would have to carefully balance reality with aspiration.
Key messages
- There are important public financial management (PFM) considerations for the New Compact, across all budget cycle phases, but particularly budget formulation.
- Providing most health aid as budget support is expected to maximise the New Compact’s transformative potential. Realising this vision will take time and will depend on the current relationship between donor and government financing, current PFM and prioritisation capacity. Substantial benefits, however, can be achieved in more mixed donor financing environments.
- Potential PFM benefits of the New Compact include strengthening the credibility and predictability of the health budget, as well as improving budget execution and monitoring by reducing unnecessary complexity in health funding flows and the burden on country systems.
- Potential PFM risks of the New Compact include high data requirements for prioritising health services and the potential to burden country systems with new responsibilities, at least in the short run.
- Implementing the New Compact will need to play on the country’s PFM strengths while circumventing (or not exacerbating) its weaknesses. It will need to be a phased approach, whilst health system and political constraints are resolved gradually.
- We recommend that the practical application of the New Compact is further explored with countries and donors and that a blueprint for implementing the New Compact is co-developed by a working group of interested parties across governments and development actors.
Health aid is volatile and fragmented, tends to displace domestic finance, relies on ineffective prioritisation, and lacks coherent transition planning and country ownership. These challenges, equally relevant to aid for sectors other than health, have long been recognised and have led to various calls for improvements. Most recently, the Lusaka Agenda calls for health aid to have a “catalytic role towards sustainable, domestically financed health services and public health functions” while emphasising country ownership and donor alignment with country priorities and systems. CGD has outlined a potential New Compact for health aid that addresses some of the long standing challenges and is aligned with the aspiration of the Lusaka Agenda.
The New Compact has implications for domestic health financing, however these haven’t been explored to date. This note aims to explore these implications with a focus on public financial management (PFM) systems and capabilities, that is, the ability for health system to clearly formulate budgets, to execute payments based on those budgets, to appropriately track agreed spending, and to monitor and evaluate spending performance.
The New Compact—What is it?
The concept of the New Compact is built on three pillars:
- Locally led evidence-informed prioritisation. Country institutions are supported to set health priorities, drawing on relevant available evidence.
- Domestic-first resource allocation. Country ownership, including financing, of the core package of high priority services.
- Consolidated supplementary aid. Donors work together and with country leaders to design a top-up package, both in terms of additional health services and other cross-cutting support.
In the approach, domestic finances support essential health services and health aid expands the package of affordable services at the margin (see Figure 1 and Box 1). Instead of targeting the most cost-effective services, donors support countries to have effective prioritisation processes and direct any additional financial support to health services that would otherwise not be covered by domestic funds. This approach encourages better planning and prioritisation by countries and donors, leading to more health for the money. As countries’ health financing is expected to improve and domestic financing includes more priority services, health aid focused at the margin is naturally crowded out, offering a gradual, coherent aid exit strategy for thriving countries and ensuring the sustainability of financing for countries that continue to need support. Perhaps most fundamentally, it empowers national decision makers and national policy processes.
The New Compact does not:
- Prescribe in detail which health services should be financed, by whom and how. It provides organising principles and a starting point for making these decisions consistently over time to improve health financing in line with countries’ priorities.
- Rule out the possibility of government-donor joint co-financing specific health services.
- Instruct how health aid should be channelled in a particular context e.g., on- or off-budget.
- Amount to or require introducing specific reforms in the countries’ health financing systems, although there are mutual synergies between the New Compact and good financial management (more on this below).
Figure 1. Illustration of prioritised health benefits package with aid investment at the margin
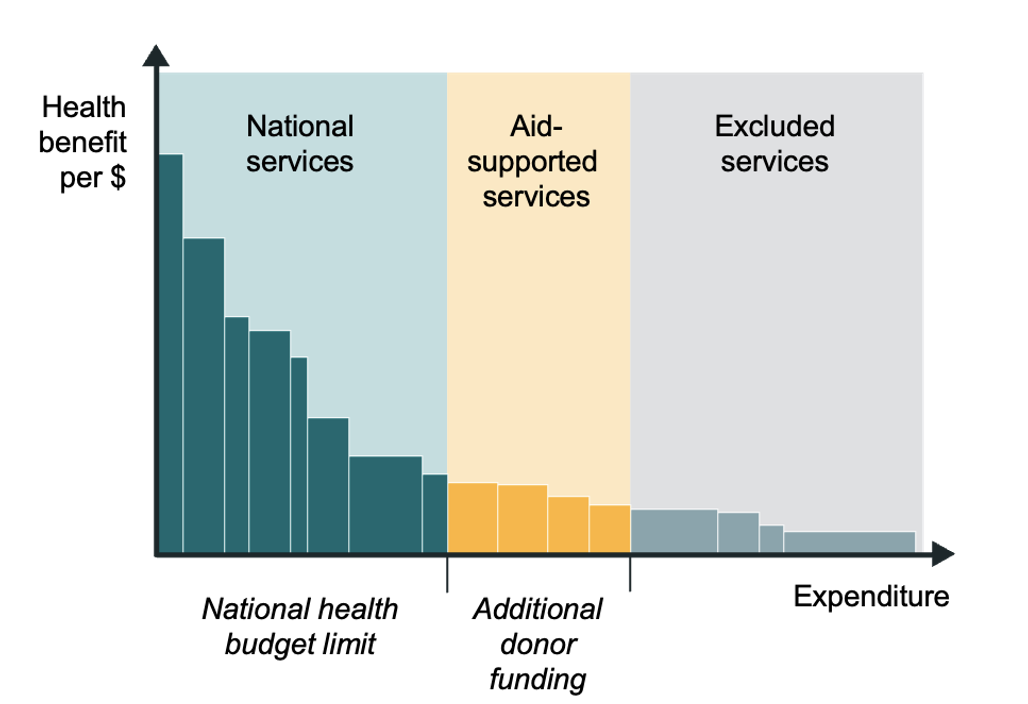
Box 1. Essential terminology in the New Compact
Health benefit package refers to the selection of health services that is being provided, at a certain coverage of costs and population.
Prioritisation refers to arranging service delivery activities, services or programmes, hereafter “health services” (e.g., measles vaccination, antiretroviral therapy for HIV, aspirin for CVD secondary prevention), in decreasing order of priority based on their expected value per dollar spent. A straightforward way of capturing the value of health services is by measuring/estimating the units of health benefit (e.g., lives saved, DALYs averted) per dollar spent; in practice, the notion of value is context-specific and can include additional considerations, such as equity.
Core or essential refers to the health services with the highest priority i.e., which provide the best value, up to the limit of the domestic health budget.
Marginal or top-up refers to the health services prioritised just after (or which provide “next best” value compared to) the core or essential health services.
The New Compact—How to rearrange funding flows?
The vision of the New Compact is one of country-prioritised health aid delivered in increasing alignment between donors and government budgeting processes—echoing the Lusaka Agenda’s aspiration “to align behind one national plan, one budget, and one monitoring and evaluation system, and enabling pooled and joint financing approaches to support core health system objectives.” The New Compact supports the “one plan” part of aspiration and to some extent the “one budget.” Linking the core unified health benefit package resulting from prioritisation to the health budget reconciles how health aid is usually organised—around priority services—with how domestic health financing is usually structured—around service delivery platforms e.g., primary health care and health care functions e.g., prevention and treatment.
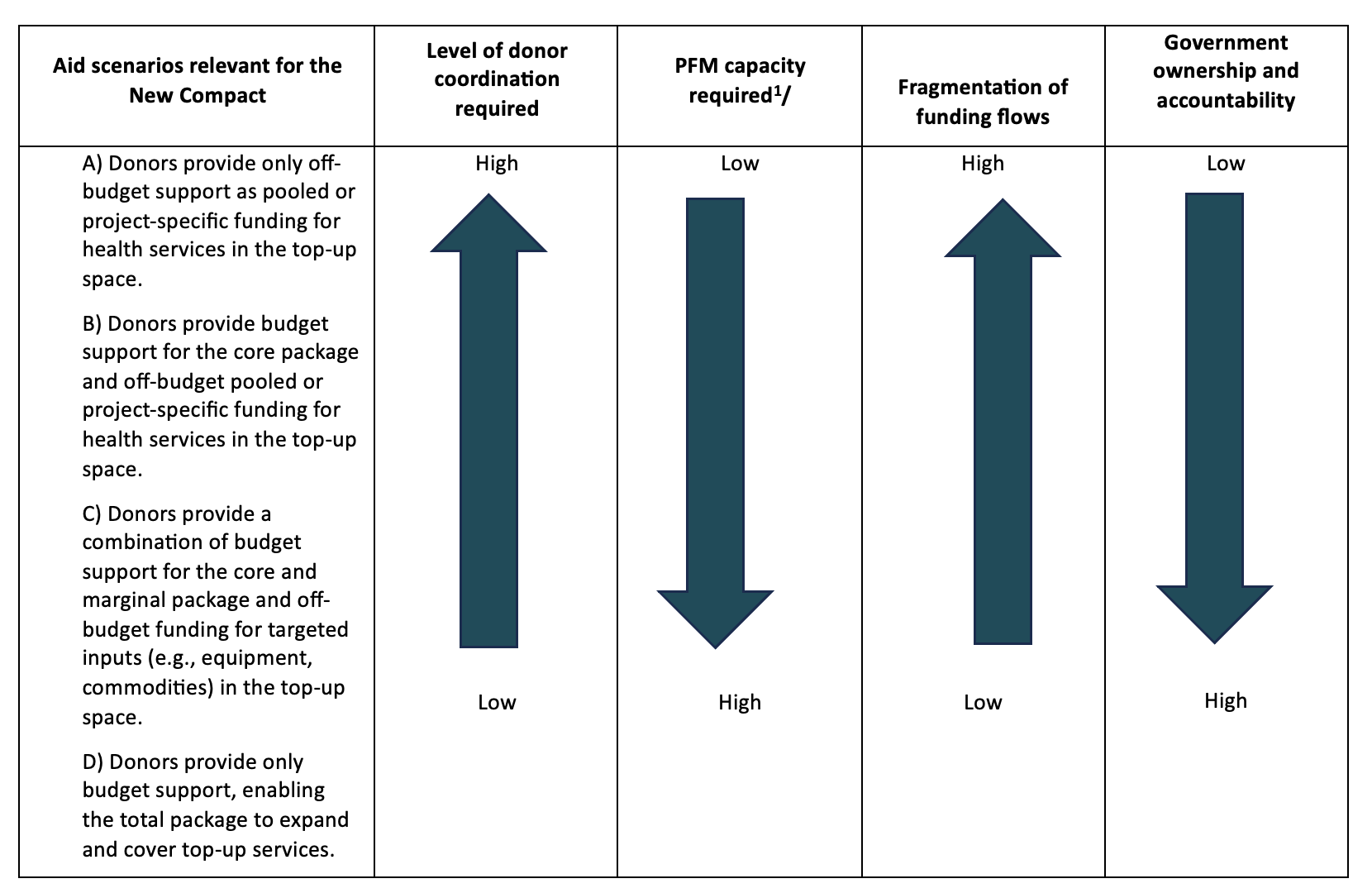
However, realising the vision of the New Compact may not be immediately achievable in all settings and may, in part, depend on confidence in country PFM capabilities. That is, the ability for health system to clearly formulate budgets, to execute payments based on those budgets, and to appropriately track agreed spending. Implementing the New Compact could take a range of different forms en route to a one plan, one budget vision. In Figure 2 we identify a spectrum of notional scenarios for reorganising health aid under the New Compact approach, arranged from a partial to a full implementation (again, notionally) of the New Compact’s principles. One illustrative scenario (A in Figure 2below) is where there is agreement on prioritising health services, but donor support is largely off-budget. Such a scenario would capture only a small, if essential, part of the New Compact’s potential benefits (coordinated country-led prioritisation) while maintaining the fragmentation of funding flows. This scenario would require intense coordination across government and donors for harmonising budgets, spending rules and processes, and monitoring frameworks across all financing sources. It would also act as an initial stepping stone towards more integrated approaches.
At the other end of the spectrum, in illustrative scenario D, all health aid is on-budget and focuses on expanding the total package of services, including those at the margin—the number of funding channels is largely reduced, coordination mostly concerns budget formulation, but pressure on government capacity and systems is high. While aid data from the OECD Creditor Reporting System indicate health aid delivered as budget support is and has been historically much lower than as project-specific interventions, a move in this direction would go a long way towards strengthening country ownership and reducing fragmentation.
Pragmatic scenarios in a given setting would most likely attempt to identify an implementation approach that balances gains in complexity (or reduced fragmentation), the costs of coordination, gains in government ownership, and available PFM capacity. Further contextual factors may also influence what is both feasible and desirable, such as the level of trust between government and donors, the strength of the country’s PFM system, and the government’s long-term PFM and aid agenda. Illustrative scenario D maximises, in principle, the potential benefits of the New Compact, however it may not be realistic for all countries to start implementing the New Compact directly under such a scenario; most likely this will be a journey in which practical arrangements will evolve in line with country and donor realities.
Figure 2. Illustrative scenarios of the New Compact
The New Compact and implications on PFM
The coordinated, principled reorganisation of which health services are funded by whom is the essence of the New Compact and while evidence informed prioritisation of services is a widely employed practice (particularly in high-income countries) health financing mechanisms are typically not organised by health service. For example, payments to facilities might be done on a capitation basis, where payments are linked to registered patient numbers, but not the services received. It is important therefore to understand how prioritisation of services—and the New Compact specifically—translates into implementation. To do this, the phases of the budget cycle—formulation, execution, and evaluation (see Box 2)—offer a useful guiding framework. The New Compact has practical relevance particularly to the budget formulation phase because of the essential link between prioritisation and resource allocation. Implications for budget execution and budget monitoring would depend on the practical arrangements of the New Compact (Table 1).
Box 2. Budget cycle phases
Budget formulation is the process of deciding which health services will be implemented by whom and how they will be financed. It entails two major components: budget planning, where a short- to medium-term budget plan is developed based on the expected resource envelope and macroeconomic and macro-fiscal frameworks; and budget preparation, where administrative units (e.g., line ministries) develop budget proposals, submit, and negotiate them with the Ministry of Finance (MOF) before approval by the legislature.
Budget execution involves the release of funds to line ministries or government departments/agencies according to the approved budget and making payments for goods and services. It covers the processes that determine how funds are released, where funds are banked, the approval protocols necessary for their usage, tendering and procurement, actual expenditure, and how expenditures are accounted for and reported against.
Budget monitoring involves ensuring that spending agencies and entities comply with laws and regulations, implement good financial management systems with reliable financial reports and internal controls and audits, and achieve budgetary objectives.
Table 1. The New Compact and the budget cycle
|
Phase |
Key activities |
Expected interaction with the New Compact |
|---|---|---|
|
Formulation |
Macroeconomic projections by the Ministry of Finance (MOF) determine global expenditure levels |
* |
|
Ministry of Health (MOH) prepares costed health sector plan and submits budget proposal |
*** Cornerstone of the New Compact approach. Costs and expected benefits of the activities in the plan are estimated jointly by the government and donors and inform the jointly agreed prioritisation. Translating the prioritisation exercise into the health budget would have to consider other PFM aspects e.g., budget classification used; which institution has authority for capital and recurrent spending; special spending rules for specific inputs. |
|
|
Negotiations between MOH and MOF |
** Strengthens MoH position as having greater control of health system resource allocation, including from external sources. Strengthens value for money domestic financing for health and therefore pitch to MoF for budget. |
|
|
Final budget debated, amended, and approved in/by Parliament |
* |
|
|
Execution |
Budget is released from Treasury to MOH. Donors may deposit on-budget funds in a ring-fenced central bank account or may use commercial banks. |
** The extent of changes required at these levels would depend on the extent to which aid is provided as on budget support—see also Figure 2. Examples of areas that may be impacted include: where and when health aid funds are banked; tendering and contracting goods and services; payroll management; committing, authorising and releasing funds; capacity of frontline providers to implement changes in the nature of financial transactions. Such areas would have to be identified early on in planning the roll-out of the New Compact approach. |
|
Expenditure is committed to goods and services. |
||
|
Goods and services are acquired. |
||
|
Payments are authorised and released to suppliers of goods and services. |
||
|
Financial transactions are recorded in the Financial Management Information System. |
** Monitoring the implementation of the New Compact requires consistent, comprehensive, and integrated recording of financial transactions. |
|
|
Monitoring |
Supreme audit institution (SAI) monitors public spending against stated budgets and spending targets and ensures accordance with relevant laws and regulations. Off-budget spending may be audited by other audit institutions. |
** Largely dependent on government-donor alignment in formulation and execution. Ideally all health spending is audited at consistent schedules by the same institution. |
Source: the authors; Key Activities based on Budgeting for Health (Chapter 8 in Strategizing national health in the 21st century: a handbook), Budget Execution in Health - Concepts, Trends and Policy Issues; and Following the Government Playbook Channeling Development Assistance for Health through Country Systems.
Notes: * denotes limited or unlikely interaction with the New Compact; ** denotes likely interaction depending on how the New Compact is realised (see also Figure 2); *** denotes crucial interaction or changes as a result of the New Compact.
The New Compact and the PFM system—benefits and risks
Despite longstanding reform attempts, many countries continue to face multiple weaknesses and challenges in their PFM systems. At the same time, PFM practices are also evolving, with COVID-19 providing a springboard for reflection on focus areas for PFM development. Adopting the New Compact could support PFM strengthening along several lines (Table 2). For budget formulation, it promises to simplify and stabilise health funding flows while also increasing the health budget’s credibility by introducing clear principles and evidence-informed practices to decide who pays for what in the health sector, as well as justifying the total amount requested from the Ministry of Finance. Moreover, planning health funding in terms of health services would provide further arguments for accelerating the implementation of programme-based budgeting as a more flexible, effectiveness-oriented approach to managing the health budget. These benefits create the premise for improvements in budget monitoring and execution: having fewer funding flows organised by clear principles can reduce complexity and duplication in monitoring financial transactions; improve accountability by consolidating and clarifying the financial accountability framework; and reduce the administrative burden of financial management at all administrative levels—all leading to clearer, more timely, more actionable budget monitoring outputs.
The extent to which these benefits can be realised will depend, in practice, on the current state of the country’s PFM system and on the policy choices made jointly by countries and donors under the auspices of the New Compact i.e., the practical arrangements governments and donors will make to reorganise health funding. The New Compact is neither a magic bullet, nor does it work in a vacuum. It is crucial that an appropriate initial scenario of the New Compact is identified. Indeed, it may well be the case that the New Compact is more challenging in settings where PFM systems do not have a certain level of maturity or where donors and countries are only partially willing to engage with principles of the approach. Moreover, even where the New Compact is desirable and implementable, reaping the maximum benefits may not be within reach in the short-term, but a principled, predictable trajectory of successive scenarios and practical arrangements may be identified. Once the health prioritisation is agreed upon, a roadmap of funding arrangements can be drawn up to consider health system (financing, human resources, commodities, physical infrastructure, information systems), PFM, macroeconomic and external funding realities, and expected developments. Tailoring the vision of the New Compact to these realities and constraints will likely be a multi-year process, with initial arrangements followed by continuous dialogue and gradual practical developments.
There are also potential risks to adopting the New Compact (also Table 2). We argue these risks can be managed if anticipated well in advance and by making transitional arrangements to avoid overburdening existing systems and disrupting frontline services e.g., joint government-donor funding may continue for selected services or programmes on a time-bound basis until appropriate capacity is strengthened. It is important to reiterate that the result of prioritising health services should be used as a guide, not as an absolute prescription, and the New Compact entails a progressive realisation based on realities on the ground.
Table 2. Benefits and risks to PFM of introducing the New Compact
|
Budget cycle phase |
Potential benefits of introducing the New Compact |
Potential risks of introducing the New Compact |
Risk mitigation strategies |
|---|---|---|---|
|
Formulation |
|
|
|
|
Execution |
|
|
|
|
Monitoring |
|
- Channelling more funds through government systems may increase the risk of misappropriation in the absence of strong PFM systems. |
|
Next steps
The New Compact is expected to work with and be embedded within the countries’ existing health system and PFM realities. However, a well performing PFM system can facilitate the adoption and maximise the benefits of adopting the New Compact. Making the New Compact a reality will take more than an analytical exercise of prioritising health services. It will also entail thinking through how changes to funding health services will translate into the health budget and, ultimately, into service delivery.
A key next step will be to develop the blueprint governance arrangements for making the New Compact a reality, which would map out its range of implications and guide how to bring together a range of stakeholders and specialists from across disciplines (health financing and PFM, but also governance and programme delivery). This can also include developing the principles and overall structure for a roadmap/practical toolkit for adopting the New Compact as a practical instrument to guide countries and development partners. This can use available tools for diagnosing existing challenges to PFM in health (e.g., UNICEF, FinHealth), as a way to structure detailed considerations and policy options.
Topics
CITATION
Gheorghe, Adrian, Pete Baker, Javier Guzman, and Tom Drake. 2024. A New Compact for Health Aid: Integrating Evidence-Informed Priority-Setting and Public Financial Management. Center for Global Development.DISCLAIMER & PERMISSIONS
CGD's publications reflect the views of the authors, drawing on prior research and experience in their areas of expertise. CGD is a nonpartisan, independent organization and does not take institutional positions. You may use and disseminate CGD's publications under these conditions.
Thumbnail image by: sorapop / Adobe Stock



