Recommended

Blog Post
Pandemic Proof: Evaluating the Monkeypox Response
Blog Post
Monkeypox: Infectious Disease Response Déjà-Vu
This blog was first published by Health Policy Watch on August 23, 2024.
With the number of new mpox cases continuing to rise, and many more potentially undetected, African countries affected by the latest outbreak are racing to mobilize funds and urgently deploy medical countermeasures, including vaccines. As the current epidemic unfolds, there is an undeniable feeling of déjà vu. Global efforts are falling short of what is needed to mount an urgent, well-coordinated response to curtail the crisis.
The world learned several lessons from COVID-19. But barring some areas of incremental progress, these lessons have yet to be translated into concrete actions.
Below we look at the global response to the latest mpox outbreak to date, zooming in on three specific dimensions.
1. Emergency declaration: a more proactive approach with empowered regional decision-making, though questions remain
On August 13, the Africa Centers for Disease Control and Prevention (Africa CDC) officially declared the ongoing mpox outbreak a Public Health Emergency of Continental Security (PHECS). This was the first time a regional institution had made such a declaration, marking a significant milestone in the empowerment of African institutions to lead and coordinate responses to public health threats.
The World Health Organization’s (WHO) declaration followed the next day. The decision, meant as a signal to donors to step up resources to curtail an outbreak, was made earlier than in previous outbreaks. In comparison, during the 2022 mpox outbreak, the declaration came after approximately 16,000 cases were reported across 75 countries. In contrast, the 2024 declaration was made before the virus had spread beyond Africa, signaling a more proactive approach.
But there is still a need to improve the “trigger” mechanism and shift from a binary approach to an epidemic scale that reflects the severity of a pathogenic outbreak. And while the regional and global declarations were aligned in this case, questions remain about what happens if decisions do not sync up.
2. Surge financing: incremental progress but not yet fully operational
The need for adequate surge or at-risk financing is arguably one of the most salient lessons from COVID-19. G7 and G20 leaders have recognized its importance and several funds and initiatives, including various Development Finance Institutions and the Africa Epidemics Fund, have signaled support, yet there is still little, if no, money flowing.
Gavi’s $500 million First Response Fund that makes resources immediately available for outbreak response is an exception. The Fund was approved by its board in June 2024, so Gavi could theoretically start drawing on these resources. However, these funds can only be used for vaccines, not other medical countermeasures, and regulatory barriers are creating hurdles. The mechanism can only procure vaccines that have received WHO emergency use listing, even though two available mpox vaccines (MVA-BN and LC16m8) have already been approved by several well-resourced regulatory authorities (see Table 1).
In the short term, Gavi and other global health initiatives should revise procurement policies to recognize approvals from WHO-Listed Authorities—a new framework established by WHO to identify mature regulatory bodies operating at an advanced level of performance.
Surge financing should also be deployed to contract for manufacturing capacity. Specifically, Denmark’s Bavarian Nordic and Japan’s KM Biologics that produce the two mpox vaccines recommended by WHO could use third party facilities to ramp up production (see Table 1).
The current outbreak underscores the need for donors to continue to work towards a more coordinated and coherent surge financing facility covering a range of health products and uses (this could entail building upon existing mechanisms rather than creating new ones).
3. Procurement and delivery strategies for medical countermeasures: urgent calls for what’s needed but the response is slow to start up and fragmented so far
We already have safe, efficacious vaccines to prevent mpox. But at roughly $100 a shot for a two-dose regimen (MVA-BV), the vaccines are expensive. The immediate priority should be getting as many of the 10 million vaccine doses needed, as estimated by the Africa CDC, procured and delivered to affected countries in Africa.
Donated doses can help fill immediate gaps. The DRC whose regulator recently granted emergency use for two vaccines now expects to receive donated doses from the EU, US and Japan shortly. Additional announcements are trickling in. Now is the time for countries holding stockpiles to step up and share supply with the most affected countries to curtail further spread (see Table 1 and Figure 1).
Figure 1. Snapshot of estimated vaccine needs in Africa compared to latest tally of available doses and donation announcements [updated as of August 22, 2024]
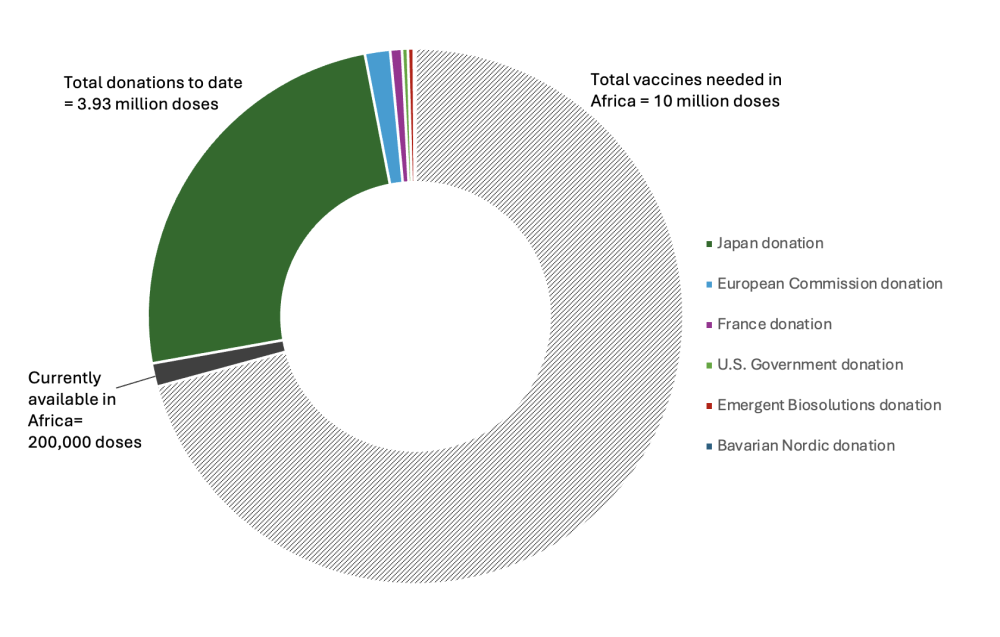
Sources: https://africacdc.org/news-item/european-commission-coordinates-procurement-and-donation-of-215-000-vaccine-doses-from-bavarian-nordic-to-support-africa-cdc-in-addressing-the-mpox-outbreak-in-africa/; https://www.gavi.org/vaccineswork/will-vaccines-help-stop-mpox-outbreak-africa. See Table 2 for breakdown of donation tally and sources.
But dose donations will require extremely close coordination to manage the myriad legal, regulatory, logistical barriers involved. In leading this effort, Africa CDC should partner with Gavi, drawing on its experiences coordinating COVID vaccine donations.
Last week, Bavarian Nordic indicated it has capacity to manufacture 10 million doses by the end of 2025, including up to 2 million doses by end 2024. Activating pooled procurement mechanisms, backed by financing from donors alongside African regional entities and countries, to coordinate purchasing should be a critical component of the global effort.
Delivery of medical countermeasures was another shortcoming of the COVID response. Specifics of the current outbreak pose particular challenges for delivery: transmission mechanisms and target populations differ from previous mpox outbreaks; ongoing conflict in the most affected areas; and vaccines are either delivered in multiple doses or using a method that a lot of vaccinators are not familiar with. Global health institutions, including Gavi, UNICEF, and WHO, also need to work closely with other partners, including humanitarian organizations and multilateral development banks, like the World Bank, to leverage their financing to support delivery and related response needs.
Finally, there are additional R&D needs. Usage of Bavarian Nordic’s MVA-BN vaccine is currently limited to adults, underscoring the urgency to broaden usage to children and adolescents, who are disproportionately affected by the current outbreak. In addition to vaccines, R&D is needed for rapid, point-of-care diagnostics and treatments.
While these immediate priorities should be top-of-mind, longer-term efforts can help down the line. Gavi’s new Vaccine Investment Strategy, approved by its board in June 2024, includes plans to set up a global stockpile.
Bavarian Nordic has also reportedly entered into an agreement to transfer technology to select African manufacturers. While important, announcements around diversifying manufacturing via technology transfer agreements will not materialize doses needed in time to curtail the current outbreak.
World leaders must respond to the calls for strong coordination and immediate access to medical countermeasures. If not, the evaluations and after-action reviews of the international response to this latest mpox outbreak will read as the same story of inequitable access that characterized the COVID-19 pandemic.
With thanks to Rosie Eldridge for research support.
Table 1. Summary of two vaccines recommended by WHO
|
Vaccine |
Manufacturer |
Vaccine type |
Dosing/schedule |
Indication |
Regulatory approval status |
Existing trials |
|---|---|---|---|---|---|---|
|
MVA-BN(Modified Vaccinia Ankara - Bavarian Nordic) Marketed asJynneos (US, Switzerland), IMVANEX (Europe, UK), IMVAMUNE (Canada) |
Bavarian Nordic, Denmark |
Live, attenuated, non-replicating vaccineproduced from Modified Vaccinia Ankara (MVA) virus |
Recommended for adults ≥18 yrs) and at-risk, immunocompromised individuals |
Only mpox vaccine with widespread regulatory approval, including from US Food and Drug Administration (FDA) and European Medical Agency (EMA) Only two African countries (DRC, Nigeria) have granted Emergency Use Authorization WHO has recommended undergoing the Emergency Use Listing (EUL)process |
The safety and efficacy in children (≤18 years old) have not been established,but are being studied |
|
|
LC16m8 |
KM Biologics, Japan |
Live, attenuated, replicatingvaccine produced from Modified Vaccinia Ankara (MVA) virus |
Single doseadministered via dermal scarification |
Recommended for use in children and at-risk, immunocompromised individuals (only smallpox vaccine approved for use in children) |
Approved in Japanfor mpox and smallpox WHO recommends its use for mpox outbreak and has recommended undergoing the Emergency Use Listing (EUL)process |
Table 2. Vaccine Donation Announcements [updated as of August 22, 2024]
|
Donor |
Vaccine Type |
Quantity Donated |
|---|---|---|
|
Japan |
LC16m8 |
|
|
European Commission |
MVA-BN |
|
|
France |
||
|
US |
MVA-BN (JYNNEOS) |
|
|
Emergent Biosolutions |
ACAM2000 |
|
|
Bavarian Nordic |
MVA-BN |
|
|
TOTAL |
3.93 million |
Additional notes:
Kenya’s Ministry of Health also announced plans to procure MVA-BV vaccine doses from Bavarian Nordic by the end of 2024.
Bavarian Nordic plans to supply 440,000 MVA-BV vaccine doses to an “undisclosed European country”.
Topics
DISCLAIMER & PERMISSIONS
CGD's publications reflect the views of the authors, drawing on prior research and experience in their areas of expertise. CGD is a nonpartisan, independent organization and does not take institutional positions. You may use and disseminate CGD's publications under these conditions.
Thumbnail image by: Adobe Stock



