Recommended


Blog Post
The 2024-2025 Replenishment Traffic Jam
This month sees the ramping up of the World Health Organization’s (WHO) first ever Investment Round at the UN General Assembly, aiming to secure an additional US$7.1 billion for the four-year 14th General Programme of Work (GPW 14). Like a game of snakes and ladders, this presents a golden opportunity for WHO and its member states and donors to climb the ladder to flexible and sustainable financing or—if mishandled—slide down the snake to more restrictive funding.
In this blog, we summarise WHO’s current financing model and its shortcomings, and note that the Investment Round is more likely to be a success if WHO is able to demonstrate improvements in how it will govern the use of flexible resources and prioritises raising flexible funding over more funding. Success will also be bolstered if member states that support flexible funding, as well as first time voluntary funders, announce their pledges early to increase momentum.
WHO financing—too little, too inflexible, and undemocratic
WHO is inadequately financed to respond to the numerous health challenges in today’s rapidly changing world. Its 2022–2023 biennial budget was just US$6.72 billion, during a global pandemic, whilst the Gates Foundation spent more than US$15 billion over a similar time period.
WHO is partly funded through predictable and flexible assessed contributions (ACs), calculated primarily on a country's GDP. But 88 percent of its funding is from heavily earmarked and unpredictable voluntary contributions (VCs). The nature of these VCs means over 60 percent of its financing originates from only nine donors.
Thus, WHO has too little resources, too little direct control over the objectives of the majority of its funds, and faces inappropriate influence over the direction of the organisation by a few major donors.
Increasing assessed contributions to liberate WHO
For an ostensibly democratic organisation responsible for setting global health priorities and improving health in all its forms, a more sustainable and flexible model of financing is critical. There was a step in the right direction at the World Health Assembly (WHA), in May this year, when a landmark decision was made by member states to adopt new sustainable financing arrangements for WHO and shift towards 50 percent of WHO’s base programme segment of the budget coming from ACs by the 2030–2031 budget cycle, at the latest.
While getting agreement on reaching 50 percent of base programme funding from ACs is a major success, it is important to note that moving towards this target will occur over time and is dependent on future WHA agreements. The current decisions also leave the majority of the budget dependent on VCs. For instance, under the current Investment Round (2025–2028), we estimate that WHO expects member states to contribute a total of US$3.7 billion of ACs out of a total of US$11.1 billion requested to deliver the drafted Fourteenth General Program of Work. Table 1 shows what this means for major WHO funding countries.
Table 1: Estimates* of the expected ACs from the top contributing member states for the proposed Investment Round (2025–2028).
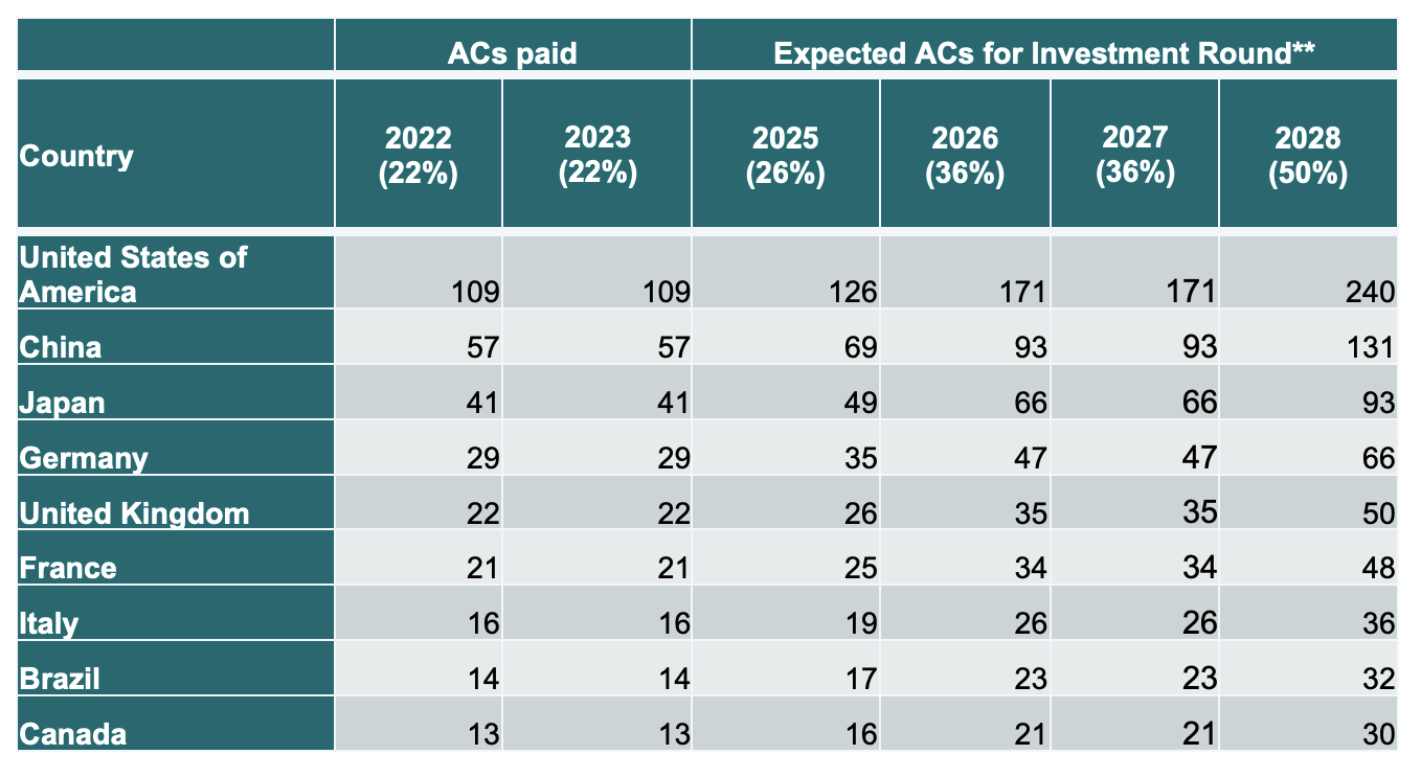
* Millions in USD. Calculated based on values from the Bureau proposal, using scaled assessments referenced in WHA74.32; estimates have been rounded.
**Percent of the 2022–2023 base budget that the ACs will make up is listed in brackets
For the investment round to be a success, member states must climb the ladder to make Voluntary Contributions more flexible
As countries consider their response to the WHO Investment Round, they must factor in not just the amount, but how far up the ladder they can climb towards WHO flexibility (Figure 1). There are three main types of voluntary funding for countries to choose from (specified VCs, thematic VCs, and core VCs, as detailed below). The success of the investment round depends on whether WHO can shift countries up this ladder—otherwise snakes await.
Figure 1: The ladders towards flexible funding at WHO

- Specified VCs are 88 percent of all VCs and they are inflexible—tightly earmarked to specific priorities, projects, and programmatic areas and/or geographical locations that are determined by donors and must be spent within a specified timeframe. The top contributors are the US, Bill & Melinda Gates Foundation, and Germany (Figure 2a).
- Thematic VCs are 7.9 percent of all VCs and are partially flexible. They are assigned for strategic engagement funding areas specified by funders, e.g., polio eradication or geographical regions, e.g., Africa. This source of funding is dominated by Germany and the European Commission (see Figure 2b).
- Core VCs are 4.1 percent of VCs and are unconditional and fully flexible. In the biennium of 2022 and 2023, only 14 funders contributed in this flexible manner, with the UK being the largest by a significant margin at over US$230,000 (Figure 2c).
Figure 2a: Top contributors of specified voluntary contributions.

Source: WHO.
Figure 2b: Top contributors of thematic voluntary contributions.

Source: WHO.
Figure 2c: Top contributors of core voluntary contributions.

Source: WHO.
Snake 1: Putting quantity of funding before quality of funding
The risk of the Investment Round is that the desire to fill the large funding gap in economically challenging times could tempt WHO to lobby for any increases in funds, rather than focus on securing sustainable and flexible streams of funding. This is likely to involve WHO increasing its dependency on the richest member states and donors. Both issues may perpetuate the existing structural defects in WHO’s funding. It is vital that WHO avoids this temptation, seeks to broaden the number of funders, prioritises fundraising for long-term flexible funding, and discourages specific funding. WHO reforms to expand the definition of thematic voluntary contributions to create greater programmatic and geographic flexibility will help, enabling contributors to pledge more flexibly.
However, it is not just down to WHO. First-time voluntary donors will need to step up, for instance at the regional Investment Round events, and show willingness to contribute, as 14 African countries did in August, by pledging over US$45 million.
Snake 2: Failing to reassure donors of the value for money and implementation of GPW14
Donors are only likely to contribute flexible funding if they believe an organisation is governed well, and has a clear, costed, and prioritised work programme.
GPW 14 outlines how WHO will enhance its end-to-end approach to results-based management, including an updated results framework and improvements to data collection and management with an emphasis on accountability and transparency measures. However, it is not clear how WHO’s governance mechanisms will adapt to managing increased flexible funding, nor how WHO will achieve its “differentiated country support model.” More concerning perhaps, is its prioritisation and costing of GPW 14 which is still set to be “preliminary” at the date of the major Investment Round summit in November this year. If this document is unconvincing in terms of prioritisation or plausibility, then WHO may find donors rapidly falling down the snakes into more restrictive and specific funding modalities.
Recommendations for WHO
- Ensure the Investment Round focuses on climbing the ladder to receive predictable and flexible financing, even if this means reducing the total funds raised.
- Deliver a well justified, rigorous, peer reviewed, costed and prioritised final GPW 14 in a transparent manner.
- Develop stronger and transparent prioritisation and governance mechanisms which include justifying decisions taken for funding allocations, between countries, regions, and the global level, and between topics, to reassure donors of value for money and the impact they are contributing to.
- Develop a reliable methodology to report the impact of flexible funding to convince funders of its value.
- Clearly communicate aims, plans for implementation, and timelines for organisational reform to instil confidence in donors that their flexible funds will return a more agile and effective WHO.
Recommendations for member states
- Deliver on the commitment for 50 percent AC. Member states must deliver on their commitments on increasing ACs, including reconfirming the target at the WHA in 2025. Any wavering of support will rapidly undermine the process.
- Don’t stop at the 50 percent AC targets—keep climbing the ladder. During the Investment Round, member states pledging VCs should aim to climb the ladder from specified to thematic, and thematic VCs to core, to support WHO’s goals to achieve sustainable financing. Major champions of core VCs, such as the UK, should announce their support as soon as possible, to increase momentum behind flexible funding. First time voluntary donors are also particularly encouraged to announce their pledges early because this will signal broadening of the funding base of WHO and also increase the pressure on the top existing specified funders to climb the ladder to flexible funding.
- Pass a 2025 World Health Assembly resolution calling for reform and coordination of global health funding rounds. In 2024, WHO, Gavi, the Pandemic Fund, and World Bank’s International Development Association all have their replenishment campaigns at the same time, creating a zero-sum replenishment “traffic jam.” This could be combined with plans for an accountability mechanism to track the Lusaka Agenda reforms.
Through these actions, WHO and member states can climb the ladder to flexible funding, putting WHO on the right footing to deliver on its vital global health mandate.
The authors thank George Antunes-Sherriff and Javier Guzman for their feedback on an earlier draft of this blog.
Topics
DISCLAIMER & PERMISSIONS
CGD's publications reflect the views of the authors, drawing on prior research and experience in their areas of expertise. CGD is a nonpartisan, independent organization and does not take institutional positions. You may use and disseminate CGD's publications under these conditions.
Thumbnail image by: utah51 / Adobe Stock



