Recommended


Blog Post
How Many Lives Does US Foreign Aid Save?
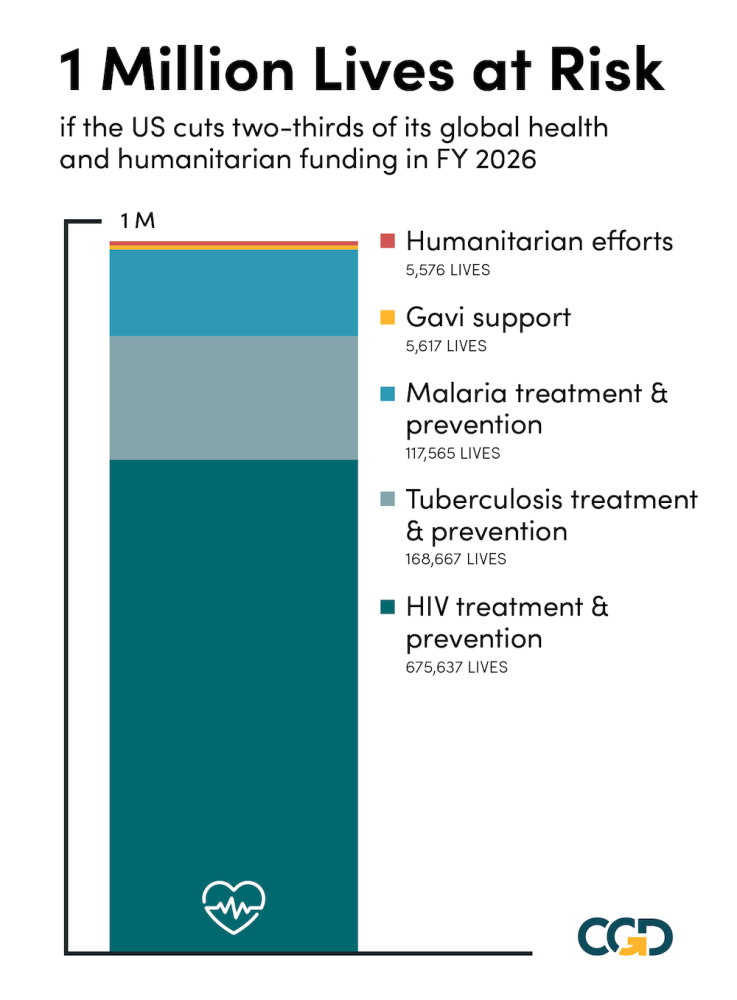
The White House has presented further details of its FY 2026 budget request. It includes a proposed two-thirds cut to global health and humanitarian funding. Such a reduction is impossible to reconcile with assurances from the administration that it is preserving life-saving assistance. A rough estimate suggests the proposed budget puts a million lives at risk.
The administration’s proposed budget suggests significant cuts across the range of global health activities, from approximately halving support for the fight against HIV, TB, and malaria to apparently zeroing out support for maternal health, nutrition, and family planning. The global humanitarian assistance budget would shrink from $8.8 to $2.5 billion (alongside a $1.5 billion discretionary trust fund for refugee and migration assistance).
Using our estimates of costs per life saved for US global health and humanitarian assistance based on available empirical evidence, we can calculate the potential number of lives at risk from such cuts. The calculation suggests the cuts could lead to 675,000 additional deaths from HIV, and a combined 285,000 deaths from malaria and tuberculosis. The total estimate is just short of one million deaths.
These numbers are open to considerable empirical uncertainty, and there are reasons to hope they would be an overestimate. There are a few different ways we could be wrong, so it’s worth breaking them down.
1. Are we overestimating the effectiveness of specific interventions that US aid finances?
It’s possible, but we think this is a comparatively small source of uncertainty. Quantitatively, HIV/AIDS drugs provided through PEPFAR and the Global Fund are the biggest contributor to our lives-saved estimates. The efficacy of antiretrovirals at extending the life-expectancy of HIV-positive patients is firmly established, and the same goes for vaccines provided by Gavi, as well as for malaria treatments and bednets financed by the President’s Malaria Initiative. So it’s unlikely the numbers are off by, say, an order of magnitude at this core level.
2. Is the administration actually just cutting fat and saving the effective aid programs?
Our underlying evidence on cost effectiveness involves average effectiveness of US assistance, not marginal effectiveness. The State Department alongside implementers could focus remaining resources on the most essential and cost-effective elements of the global health program and activities within those elements.
As an extreme illustrative exercise, if all remaining global health funding was redirected toward TB activities, which we estimate to be the most cost-effective sectoral spending per life saved, the estimated number of lives at risk from the cuts would be reduced to below one quarter of a million. We do not have (nearly) sufficient faith in either the numbers or the political plausibility to propose that.
But the idea that such significant cuts to foreign aid, particularly in health, could only cut fat is implausible. About three-quarters of that money went to HIV/AIDS, malaria, and TB, where the available evidence suggests that spending was already highly cost effective. The high-end estimates of costs per life saved from our review of foreign assistance financed interventions covering HIV, TB and malaria are between $2,000 to $5,000—compare that to estimates highly cost-effective charitable interventions that save a life for about $3,500 to $5,500. One can quibble over the precise cost-effectiveness numbers, but by any reasonable estimate you can’t cut very much from these budgets before you start reducing the number of anti-retroviral drugs, bednets, and TB tests, and people start dying.
Furthermore, the administration already went through an exercise of cutting what it saw as wasteful awards while trying to preserve lifesaving aid in the early months of 2025 (reported as ‘estimated award value cut’ in the table below). That exercise led to considerable cuts in global health and humanitarian spending but amounted to a 13 percent reduction in the humanitarian award portfolio compared to the 72 percent cut in the proposed budget, and a 20 percent reduction in the HIV award portfolio compared to a 47 percent cut in the proposed budget, for example. Again, the recissions package recently proposed by the White House would cancel previously appropriated funding to “reinstate focus on appropriate health and life spending” in the global health budget, but cuts only $900 million out of $10 billion in spending. The budget proposal for FY26 includes far deeper cuts.
3. Will other donors and recipient governments fill the funding gap?
In our earlier analysis, we spent a lot of time discussing the difference between the impact of an antiretroviral drug (life versus fairly certain death) and the impact of US aid for antiretroviral drugs, which will hopefully be partly substituted by additional financing from developing countries’ own budgets and other donors. Our headline numbers on lives saved combine both types of estimates for different sectors (malaria, tuberculosis, etc.). We have written before about how some of aid for vaccines would likely be replaced by countries’ own spending if it disappeared. But crucially, this appears not to be the case for HIV/AIDS. Hopefully things work out differently this time, but the estimates we cite of PEPFAR’s impact already build in the historical response by other governments and donors when the US was not providing the same level of support. The counterfactual we used was “no PEPFAR” specifically, rather than “no one providing ARVs at all”—but in practice, those two scenarios look quite similar.
In short, there is a lot of uncertainty here. But under a range of more optimistic assumptions, we would still end up with estimates of hundreds of thousands of lives at risk. Furthermore, these are numbers based on the more conservative evidence from available cost-effectiveness estimates (using our low-end estimates of cost-per-life-saved generates an estimate of lives lost above 2.3 million). And these numbers completely ignore the additional mortality impact of potential 100 percent cuts to maternal health, family planning, nutrition, and water and sanitation programs.
The proposed FY26 cuts are worth about 0.2 percent of federal spending, but their impact would be extreme. We hope the administration and Congress will step back from such severe cuts to life-saving assistance as the budget and appropriations process advances.
Table. Lives at risk from the proposed global health budget cut
| Actual '25 | Proposed '26 | Cost Per life saved | Lives at risk | Estimated award value cut | Proposed budget cut | ||
|---|---|---|---|---|---|---|---|
| HIV | 5,534 | 2,910 | 3,883 | 675,637 | 20% | 47% | |
| TB | 709 | 346 | 2,150 | 168,667 | 56% | 51% | |
| Malaria | 1,109 | 541 | 4,826 | 117,565 | 36% | 51% | |
| Maternal and Child (ex Gavi) | 757 | - | 92% | 100% | |||
| Gavi | 300 | - | 53,409 | 5,617 | 100% | 100% | |
| Nutrition | 165 | - | 39% | 100% | |||
| Family Planning | 608 | - | 94% | 100% | |||
| Total Global Health | 10,030 | 3,797 | |||||
| Humanitarian | 8,826 | 2,500 | 1,134,455 | 5,576 | 13% | 72% | |
| Total | 18,856 | 6,297 | 973,062 |
Notes: 2025 budget data. Global Fund budget reapportioned 49% HIV, 32% malaria, 19% TB (following our earlier piece here, which is also the source for cost per life saved). 2026 budget proposal, spending on TB/malaria calculated as total proposed spending on “prevention, treatment, control of, and research on, tuberculosis, polio, malaria, and other infectious diseases,” apportioned to the two diseases proportionate to 2025 spending. Estimated award value cut from our separate exercise here based on State Department releases
Topics
DISCLAIMER & PERMISSIONS
CGD's publications reflect the views of the authors, drawing on prior research and experience in their areas of expertise. CGD is a nonpartisan, independent organization and does not take institutional positions. You may use and disseminate CGD's publications under these conditions.
Thumbnail image by: Robert Peak/ Adobe Stock



