

The Trump administration’s recent actions on foreign aid are dramatically shifting the global health funding landscape and triggering a health financing crisis in many countries. The US is the largest global health funder, providing an estimated $12.4 billion each year. Nearly 70 percent of this ($8.5 billion) is allocated as bilateral health aid, which has been heavily disrupted by the administration’s actions. And for many of the lifesaving services supported by US assistance—from antiretroviral therapy and tuberculosis treatment to emergency care for mothers and newborns—even a temporary pause can have deadly consequences. These actions are also particularly concerning because other major global health donors, namely European governments, are slashing aid budgets and low- and middle-income countries (LMICs) are facing mounting debt pressures.
In this blog, we conceptualise this as a health system shock, present a back-of-the-envelope assessment of LMICs that are most exposed, and discuss possibilities for short-term policy responses from other funders and LMIC governments, drawing lessons from the rapid global response to COVID-19.
We find that 26 LMICs, with a combined total population of 1.38 billion, are both highly exposed to US global health aid cuts and highly fiscally constrained, meaning they are least able to adequately respond. Amid economic headwinds and shifting geopolitics, bilateral government donors as well as philanthropies and multilateral development banks may be unlikely to fill the entirety of the gap left by the US, at the necessary scale and speed. Prioritisation and agile support from funders to countries that are most exposed and least able to respond will be key.
Which countries are exposed to US global health aid cuts and fiscally constrained?
First, we consider how much US bilateral global health assistance each country receives. This encompasses funding implemented by USAID, the State Department, and other agencies, such as the Centers for Disease Control and Prevention, and which is spent primarily through US-based implementing partners. US multilateral contributions to global health initiatives such as the Global Fund and Gavi are excluded from the analysis.
To assess the magnitude of the funding shock, we compare the total amount of US bilateral global health funding that a country received to domestic government expenditure on health in 2022. We drill down on countries that are “highly exposed” to funding cuts, defined as those where US bilateral global health assistance is equivalent to 10 percent or more of government health expenditure. We then investigate two indicators as a proxy of a country’s ability to respond: their World Bank income classification and their level of indebtedness. While a full fiscal space analysis for each country would yield a more detailed picture, this back-of-the-envelope approach is designed to rapidly identify priority countries that are “highly fiscally constrained” and are therefore, in urgent need of immediate intervention by external funders.
Top countries most exposed to US funding
We find 37 “highly exposed” countries face a loss equivalent to 10 percent or more of their government health expenditure, and that US bilateral global health assistance to these countries totals $4.9 billion. This group includes considerable variation—with 25 countries facing a loss of 20 percent or more and 10 facing a loss of at least 50 percent (Table 1).
Table 1. Top 10 most exposed countries (and link to full data)
Country | Average ODA gross disbursements received from US for global health, 2022-2023 (USD millions) | US bilateral global health assistance as percent of domestic government health expenditure | Debt distress risk | Income classification | Fragile/ conflict-affected status |
|---|---|---|---|---|---|
Afghanistan | 88 | 341% | High | Low | Conflict |
Somalia | 43 | 237% | Moderate | Low | Conflict |
South Sudan | 110 | 235% | High | Low | Conflict |
Malawi | 228 | 207% | In Distress | Low | - |
Haiti | 106 | 166% | High | Lower Middle | Fragile |
Uganda | 441 | 95% | Moderate | Low | - |
Liberia | 48 | 93% | High | Low | - |
Mozambique | 414 | 83% | High | Low | Conflict |
Tanzania | 432 | 59% | Moderate | Lower Middle | - |
Sierra Leone | 32 | 52% | High | Low | - |
Source: Authors analysis of OECD CRS data (ODA in 2022 and ODA in 2023); WHO Global Health Expenditure Database; and World Bank Debt Sustainability Analysis, Classification of Fragile and Conflict-Affected Situations, and WDI data
26 highly exposed and highly fiscally constrained countries
Due to the relative magnitude of US bilateral global health assistance, the 37 “highly exposed” countries will struggle to use domestic resources to fill the gap left by the US. Within this group, we find a subset of 26 countries that are either low-income (and International Development Assistance [IDA]-eligible), or in debt distress. These 26 countries—which collectively receive $3.4 billion in US bilateral global health assistance—can be considered “highly exposed” and “highly fiscally constrained” and are exceptionally unlikely to be able to fill the gap (Figure 1).
Figure 1. 26 highly exposed and highly fiscally constrained countries that will be unable to fill the gap left by US aid
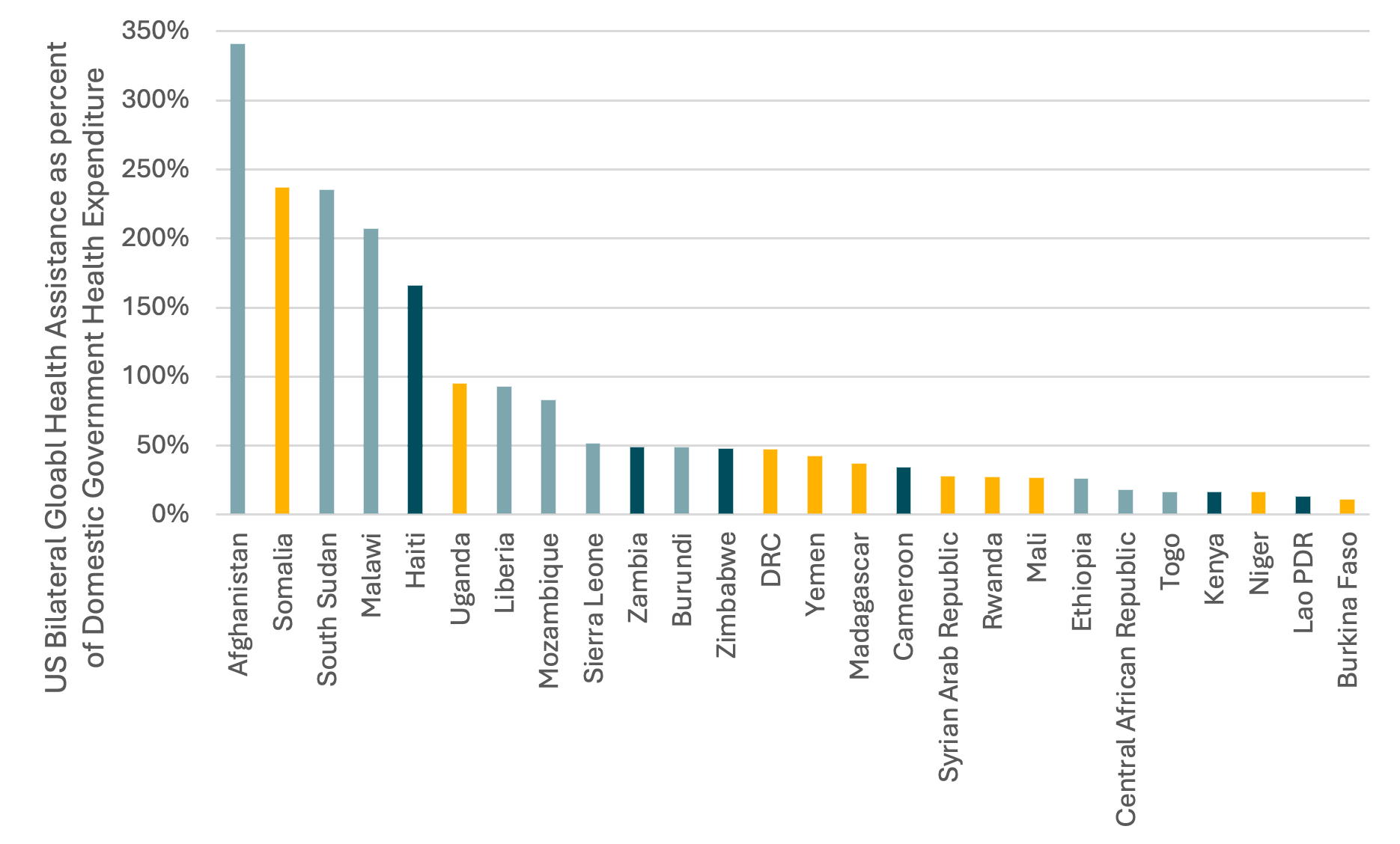
DRC = Democratic Republic of Congo; Lao PDR = Lao People’s Democratic Republic
Teal Grey = low-income country and in/at high risk of debt distress
Yellow = low-income country, not at high risk of debt distress
Teal = Lower-middle-income country in/at high risk of debt distress
US speed, financing approach, and disease focus hinders government intervention
Beyond the sheer scale of the financing gap, it will be challenging for these 26 countries to replace US support for three reasons:
- The speed of the changes. The US aid freeze is happening now, with clinics already shut. While some countries, such as Nigeria, have shown that rapid budget increases are possible, most LMIC budgetary processes are not designed to shift this level of resources so quickly and instead work around an annual cycle. During the COVID-19 pandemic, countries could, by presidential decree, launch an emergency extra-budgetary fund. But this takes time, has weaker oversight, and fails to resolve the challenge of where the funding comes from.
- The US preference to fund US-based implementers means LMIC governments would have to waive national procurement rules and contract rapidly with these implementers to maintain service delivery. It will also be challenging for the governments to know with certainty who to contract with (or how much).
- The US’s disease focus. The US, through PEPFAR, is highly focused on HIV services. Take for example the case of Uganda where PEPFAR provides ARVs to 1,416,800 people. Governments have often not yet developed the know-how or capacity to manage these kinds of services or procure these products, in large part because they are often managed by donors supra-nationally. The state is therefore unlikely to have the capacity or supply chain to rapidly scale-up.
Given this bleak picture, we review three options for how different funders can support countries to use their own resources, provide additional resources, and/or reschedule future spending into the current year.
1. Funders can support countries to use domestic resources
Countries that do wish to expand domestic financing should be supported. This is one of the few long-term, sustainable routes to fill the gap left by the US. This could include debt relief and debt pauses. For example, during COVID-19, DSSI emergency debt relief released $1.8 billion of debt repayments. This could also include urgent expansion of grants and concessional loans through the World Bank, such as the IDA crisis response window.
A catalytic option for small donors could be to provide technical assistance to countries. This could include support on executing existing health budgets, which are often underspent by 20 percent, or using rapid priority setting methods to select which US-funded services are good value for money and should be prioritised and taken over by domestic funding.
2. Funders could increase their contributions to make up the shortfall
The US provides $8.5 billion of bilateral global health aid. This could theoretically be replaced by other donors. In the initial phase of the COVID-19 response, between 2019 and 2020, non-US donors increased their contributions by over $10 billion—an unprecedented increase. However, COVID-19 was a much greater threat to high-income countries, which increased its political saliency. This current funding crisis has not triggered the same shift in political opinions, and is unlikely to dissuade European donors, such as Germany, France, Netherlands, and Sweden from cutting their aid budgets, or change the UK's newly capped aid budget at 0.3% of GDP. These donors remain focused on large competing needs, such as Ukraine, increasing defence spending, climate change, and upcoming replenishments (e.g., the Global Fund and Gavi, for which future US support remains uncertain).
A smaller scale option is to trigger emergency mechanisms and release contingency funds. For example, the UK Integrated Security Fund (UKISF) or the UK’s Rapid Response Facility. Similarly, the Global Fund could encourage countries to apply to its emergency fund. However, these are for geographically-restricted crises such as disease outbreaks and conflicts, and are not intended for this kind of large-scale, global shock in multiple countries; plus they will be rapidly exhausted.
Non-traditional donors such as China could jump in, perhaps concerned about instability and risk to repayment on $134 billion of debt. However, China only provided $783 million in global health assistance in 2023, so there would need to be a spectacular change in approach to see a significant increase. Furthermore, China plugging the gap would involve supporting a US-led global health architecture and, in the short term, funding US-based implementing partners, which is likely not politically palatable.
3. Funders (especially philanthropy) could bring forward future spend into this year
Finally, donors and philanthropic organisations could consider bringing forth future spend into this year. This could be a comparative advantage for philanthropy since they should be able to move more quickly than bilateral donors and can more easily contract US-based implementing partners. For example, in February 2020, the Gates Foundation released an extra $100 million to the early stages of the COVID response. It is notable that the annual US bilateral health budget is roughly equal to one year of the Gates Foundation total spend for all sectors including health.
Other philanthropies such as Open Philanthropy, CIFF, Buffett, Wellcome Trust, and Pivotal Philanthropies have substantial discretionary resources and may wish to contribute, especially on their preferred areas such as reproductive health, malaria and climate. This piecemeal approach, however, would perpetuate many of the long-term problems with global health financing—such as fragmentation, donor-led prioritisation, and the lack of a clear exit strategy. So, while it is possible for philanthropy to make a substantial impact on the gap left by the US in the short term, it is not without risks in the medium term.
Prioritisation and coordination is the only option
Regardless of whether donors support the use of domestic financing, provide additional funding, or bring forward future funds, it is unlikely the total gap left by the US will be filled. Our initial analysis suggests that there are 26 highly exposed and highly fiscally constrained countries that could be prioritised. With more time, a substantial assessment that looks at each country’s fiscal space, their commitment to taking on the funding for the long term, their health needs, and the value for money of services, should be carried out.
As funders consider their priorities, they should be cognisant that short-term decisions now are likely to create path dependency and will determine the future shape of global health financing. Funders should have an eye on the future system they wish to build as they mount immediate response plans.
At its core, this new system must recognise that we have left the golden age of global health and are now in the age of donor volatility. Countries can no longer be at the whim of political winds in donor countries. The world needs to shift towards a more sustainable, shock-resistant global health model, such as the New Compact and as described in the Lusaka Agenda. This doesn’t necessarily mean less aid and more domestic spending: it means seeking to pool donor resources, and therefore risk, where possible, and to put governments in charge and focus domestic resources on core health services to ensure they are resilient to donor shocks.
Thanks to Justin Hurley and Erin Collinson for comments
Topics
DISCLAIMER & PERMISSIONS
CGD's publications reflect the views of the authors, drawing on prior research and experience in their areas of expertise. CGD is a nonpartisan, independent organization and does not take institutional positions. You may use and disseminate CGD's publications under these conditions.
Thumbnail image by: Van Houtte/USAID



