Recommended
As the COVID-19 pandemic takes hold in low- and middle-income countries, it will continue to amplify existing global health and development challenges and threaten hard-won gains of the past two decades. Before COVID-19, many middle-income countries were experiencing rapid economic growth and simultaneously confronting the prospect of transitioning away from donor assistance. In the face of the challenges posed by aid transition and competing priorities for health spending amidst UHC, the global health community was focused on how to sustain and expand delivery of high-quality affordable health services to meet growing demands. As the global health and development landscape is upended by COVID-19 and the associated global economic downturn, these considerations are just as prescient. In today’s context, the need for additional health financing in low- and middle-income countries is already significant. Therefore, the role of external aid in shoring up health systems is vital to prevent backsliding on global health progress. In parallel, there is increasing uncertainty around the future of development assistance. And, the path forward for aid transition is unclear; we may even see “reverse transitions” in countries that previously transitioned from donor aid.
Although specific timelines, plans, and priorities may shift, COVID-19 will only intensify pressures on already-constrained public health budgets. Low- and middle-income country governments must grapple with how to address the direct health impacts of COVID-19, minimize the indirect health effects of the pandemic on essential health services including family planning, protect health workers at the frontline, and cushion the blow from the associated economic and social shock. At the same time, these countries will likely see economic growth grind to a halt, government revenues shrink, and debt levels increase—placing significant competing asks on limited public resources. Looking ahead, decision makers will increasingly face tough tradeoffs in financing and planning for the health of their populations, including which interventions to prioritize.
In the months before the current crisis, CGD’s global health policy team partnered with Pharos Global Health Advisors to understand competing fiscal and programmatic pressures across the health sector. The research was based on case studies in Ghana, Kenya, and Bangladesh. It aimed to drill down on challenges, risks, and opportunities associated with transitions from different global health financing mechanisms, highlighting specific implications for family planning and drawing lessons from previous USAID transitions. We encourage you to read the final report and its rich findings in entirety, but in the meantime, the key takeaways below resonate more than ever.
Co-financing pressures don’t add up
The report highlights that as external support for specific health programs ramps down, and domestic co-financing requirements ramp up, enormous pressures are placed on public budgets. In most cases, family planning constitutes a relatively small share of the budget and, therefore, does not appear to be a key contributor to these pressures. However, the long-term sustainability of family planning services could suffer disproportionate negative impacts from the fiscal pressures resulting from transitions across other health areas—as well as broader shifts in development assistance for health. Further, constraints to enhanced revenue mobilization (see CGD’s research in Kenya and Bangladesh, for example) may make it challenging to secure increased domestic spending for key health programs—or even sustain current spending levels in the current context. Altogether, the case studies paint a picture of co-financing requirements and timelines across various global health donors that are oftentimes determined in isolation from each other. Without careful recognition of the potential fiscal impact of these looming transitions, health gains could be at risk, now more than ever.
Ghana
In Ghana, a study by Oxford Policy Management and the Ministry of Health projected a steep decline in external funding across six priority health programs—from roughly $248 million in 2017 to $124 million in 2025. Concurrently, co-financing requirements are estimated to increase by approximately $206 million (see Figure 1). This suggests roughly $330 million in additional resources could be needed by 2025 to account for the decline in donor support and meet increased co-financing requirements—that’s about half of the $630 million the government of Ghana spent on health in 2017. Notably, these projections are illustrative, and it’s not entirely clear if donor funds will need to, or should, be replaced 1-for-1 by government spending.
Further, while the government has created a budget line to finance procurement of family planning commodities, execution has remained a challenge. The government has also put forward a multisectoral “Ghana Beyond Aid” approach, although there do not yet appear to be strategies in place to achieve this goal in the health sector.
Figure 1. Ghana’s projected co-financing requirements: 2017-2025

Source: Cited from Pharos report; originally in MoH and Oxford Policy Management, 2018. A roadmap for sustainability and transition from external finance: mapping donor and domestic financing for the health sector in Ghana and planning for the future.
Kenya
Similarly, in Kenya, increasing domestic co-financing requirements for HIV and immunization, coupled with growing demands to treat more expensive chronic conditions like dialysis and cancer, are challenging the government’s ambitions to achieve universal health coverage (UHC) by 2022. Based on back-of-the-envelope calculations, it appears that total resource requirements for the HIV program alone far exceed the entire 2018 UHC budget. Fiscal pressures across the health sector could potentially adversely impact the family planning program, even if it makes up a relatively smaller share of the overall health budget.
Kenya is currently facing a stark contraceptive funding gap due in large part to reduced domestic financing for commodities following devolution in 2013. Available funds—from both external and domestic sources—for family planning commodities will cover just 15 percent of the estimated total need in 2020-21 (see Figure 2). In response, the government of Kenya and family planning donors are considering a matching fund arrangement for contraceptives, in which donor support will decrease as domestic spending increases over time. We’ll be watching closely to see how the contraceptive matching fund in Kenya unfolds, along with its potential implications for the feasibility and design of similar approaches to incentivize domestic spending in other countries going forward.
Figure 2. Contraceptive commodity funding gap analysis in Kenya
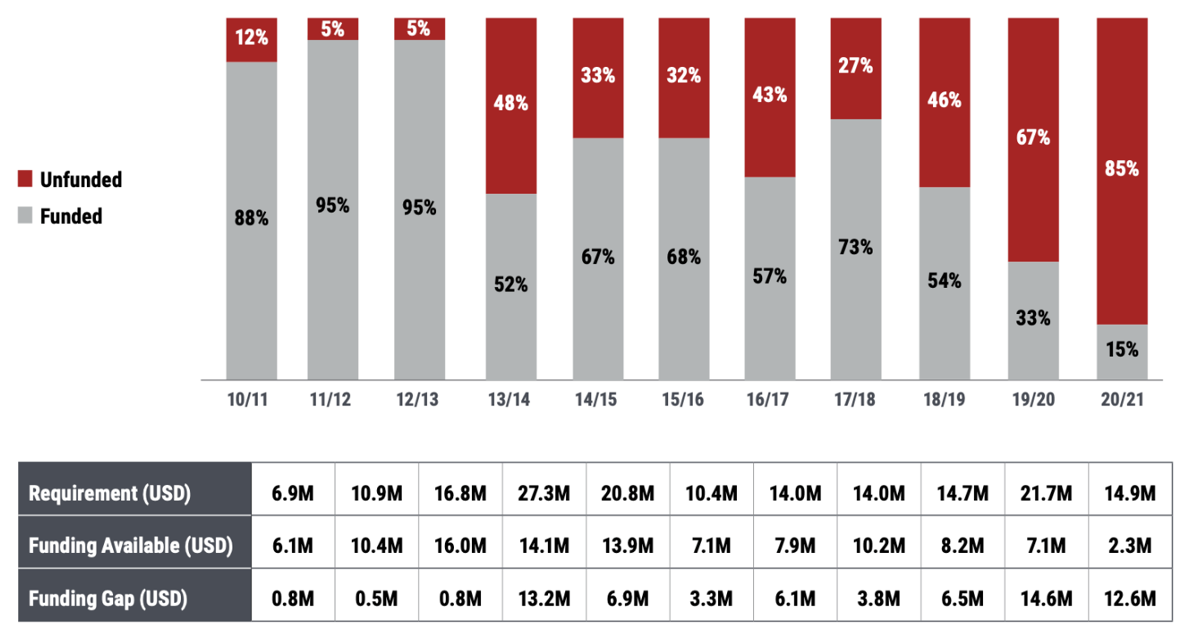
Source: Pharos report, based on CHAI 2019; FP Quantification Technical Reports 2010-2018; FP Dashboard.
Bangladesh
The government of Bangladesh, in contrast to Ghana and Kenya, covers 96 percent of family planning commodity costs, while donors and NGOs continue to fund the majority of enabling environment activities, including key population programs, quality assurance, and provider training (see Figure 3). If family planning donors were to reduce external aid in the coming years, the government may be hard-pressed to fill gaps given competing health financing needs.
Bangladesh is currently poised to enter the accelerated transition phase from Gavi in 2021 and projected to become fully self-financing in 2026. Estimates suggest that the government will have to mobilize an additional US $67 million in annual immunization spending over the next six years, nearly three times what it spent on immunization in 2017 ($24 million). Further, per our colleague Rachel Silverman’s previous estimations, Bangladesh is also projected to transition from IDA and GPEI around 2025. Even if these (simultaneous) transitions do not occur as initially projected, the impacts of COVID-19 are likely to create considerable long-lasting fiscal challenges, with important implications for the sustainability of Bangladesh’s family planning program. (For context, economic growth across the South Asia region is now projected between 1.8 and 2.8 percent for 2020, down from the initial 6.3 percent estimate before the pandemic—and potentially the lowest in four decades.)
Figure 3. Funding sources of selected family planning programmatic areas in Bangladesh, 2016

Source: Calculations from Pharos report, based on FPSA, Bangladesh 2016.
It’s not just about the money
When it comes to transitions in health aid, it’s not just about how low- and middle-income countries fund health programs but also about what they fund. Some middle-income countries may face more of a priorities ditch, rather than a financing ditch, as our CGD colleagues have argued. Therefore, government decisions about what to finance are not just a matter of resource availability. While policy choices about how to allocate resources and design benefits packages for health can be underpinned by political economy dynamics, they should more importantly be informed by a transparent and accountable priority-setting process that considers cost-effectiveness and allocative efficiency. The role of priority setting will become even more critical to stretch limited resources as far as possible during the COVID-19 response and beyond. (Check out more on CGD’s priority-setting work via the International Decision Support Initiative, which supports health technology assessment in Ghana, Kenya, and other countries.)
In the case of family planning, the divergent experiences of countries like Kenya and Bangladesh suggest that budget allocations for family planning have varied over time and across contexts, due in part to shifting priorities. Looking ahead, inclusion and provision of contraception as part of health benefits packages (HBPs) can help assure a more sustainable approach; available evidence suggests contraception is likely to be cost-neutral or cost-saving for national healthcare payers and insurers (stay tuned for more from CGD on assessing FP for inclusion in national HBPs). Donors have an important role to play in incentivizing domestic spending for the most cost-effective products and interventions. Alongside better incentives, the need to support cross-cutting functions like priority-setting, procurement and supply chains (the focus of a recent CGD working group), and public financial management is also abundantly clear.
Charting a way forward... together
The evidence is piling up—a piecemeal approach to managing the broader set of fiscal pressures and uncertainties will put progress towards universal access to voluntary, affordable, high-quality family planning at risk. The report findings echo previous research in underscoring the importance of a more holistic and coherent approach at the global and national levels—a shift that will require many global health partners to move beyond narrowly focusing on their own specific disease and/or program areas.
Looking ahead, as donors roll out mechanisms to incentivize and promote greater domestic spending for health programs, they should do so in collaboration with government counterparts and other development partners to make their asks realistic given each country’s fiscal situation. Country policymakers and donors would also benefit from co-creating assessments, timelines, and plans that include transparent data on the cost and impact of programs so that governments have visibility into what they will need to finance in the absence of external aid.
The exact recipe for how to set into motion a more coherent approach is far from straightforward, but the report touches on the essential ingredients. For example, engaging private sector actors will be critical, especially considering that many women and girls in middle-income countries rely on the private sector to access contraceptives; in countries like Ghana, Kenya, and Bangladesh, an estimated 40 to 50 percent of all users obtain contraceptive supplies in the private sector. Further, ensuring that family planning is included as part of sector-wide planning, budgeting, and prioritization at the national level will be important. But this approach is not without challenges; the family planning community will need to have champions to ensure its voice is not “diluted” in a broader sector-wide approach. At the international level, the Global Action Plan’s Financing Accelerator and UHC 2030, for example, aim to enhance global coordination on transition; although these efforts still appear nascent and their effects on charting a different path remain to be seen.
The landscape of aid transition in health is nuanced, complex, and unclear—and the pandemic will only intensify existing uncertainties and competing asks on public budgets. Before COVID-19, the challenges, as illustrated by the case studies, were already significant: Ghana needed to raise additional resources equal to roughly half its total health spend to meet transition requirements; Kenya was facing an 85 percent financing gap for contraceptives; and Bangladesh required a near tripling of immunization spending over the next six years. Now, in the face of COVID-19, these and other countries will also face reduced government revenues, rising debt levels, and uncertain levels of development assistance, among other shifts. The need for a reimagined approach to aid transitions and broader uncertainties in global health aid, with a greater push for sustained external support, is clear. Out of this unprecedented crisis, there is an opportunity to forge a new path forward: not disease-by-disease, but together across health systems.
Many thanks to Felice Apter, Kalipso Chalkidou, and Cassandra Nemzoff for helpful feedback, and to colleagues at Pharos Global Health Advisors for collaboration on this project.
Topics
DISCLAIMER & PERMISSIONS
CGD's publications reflect the views of the authors, drawing on prior research and experience in their areas of expertise. CGD is a nonpartisan, independent organization and does not take institutional positions. You may use and disseminate CGD's publications under these conditions.
Thumbnail image by: Yagazie Emezi/Getty Images/Images of Empowerment



