Recommended
In late February, UK Prime Minister Boris Johnson launched a government-wide “integrated review.” The review, described as “the biggest review of Britain's place in the world since the end of the Cold War,” will report directly to the prime minister. Unlike its more narrowly focused predecessors, this review will cover not only the Ministry of Defence, but also the Foreign Office and the Department for International Development, as well as other departments, including the Home Office, Treasury, and the Department for Business, Energy and Industrial Strategy. Its cross-government approach is central to the UK’s Fusion Doctrine, which aims to fuse the government’s economic, security, and influence capabilities to build a stronger, more coherent approach to national security. Why then is health missing from this review?
The integrated review is a unique opportunity to rethink the UK’s role in a changing and increasingly interconnected post-Brexit world. (It’s akin in ambition and scope to the US Department of State’s Quadrennial Diplomacy and Development Review, last carried out in 2015.) And though the integrated review is much broader than global health, at a time when COVID-19 is claiming its toll on lives, trade, and the global economy, the review offers a valuable vehicle for articulating a holistic vision of how the UK can best deploy its resources to enhance national security, while also improving health at home and around the world. Below we outline the opportunities for including health measures and building global health into the national security objectives at the core of the Fusion Doctrine.
Public health and national security risk assessments, past and future
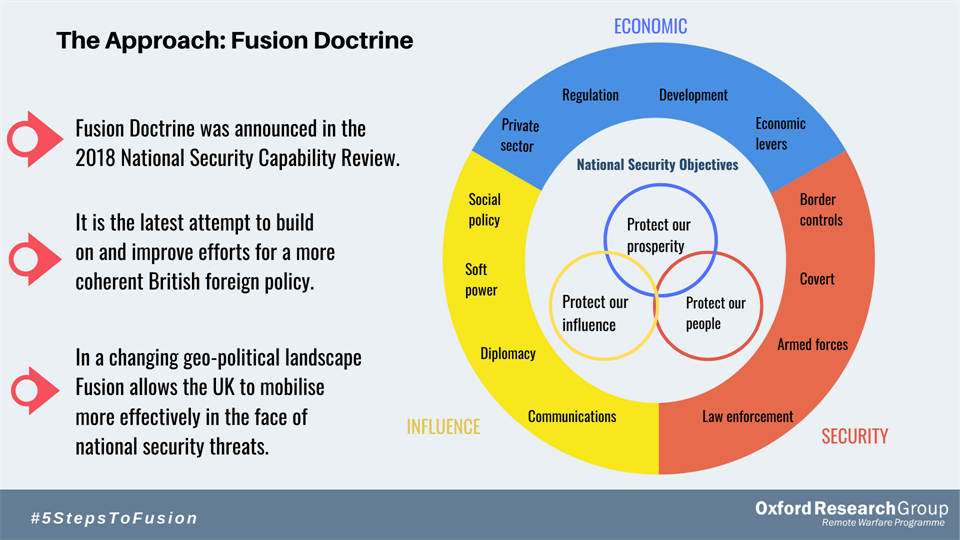
Since 2010, government security reviews have included national security risk assessments. These assessments have tended to identify major public health emergencies and major natural hazards as Tier 1 risks, with implications for health in the UK and across the world. However, as in past such exercises, the role of global health as a UK national strategic capability within the Fusion Doctrine was relatively overlooked in the 2018 National Security Capability Review and its economic prosperity, security and influence objectives. The 2018 Review only briefly mentions antimicrobial resistance, the now acutely topical issue of pandemics, and UK-based emergency health team interventions during terrorist incidents and humanitarian disasters within or beyond UK borders. The graph below demonstrates the priorities set out in the Fusion Doctrine, where health is notably absent.
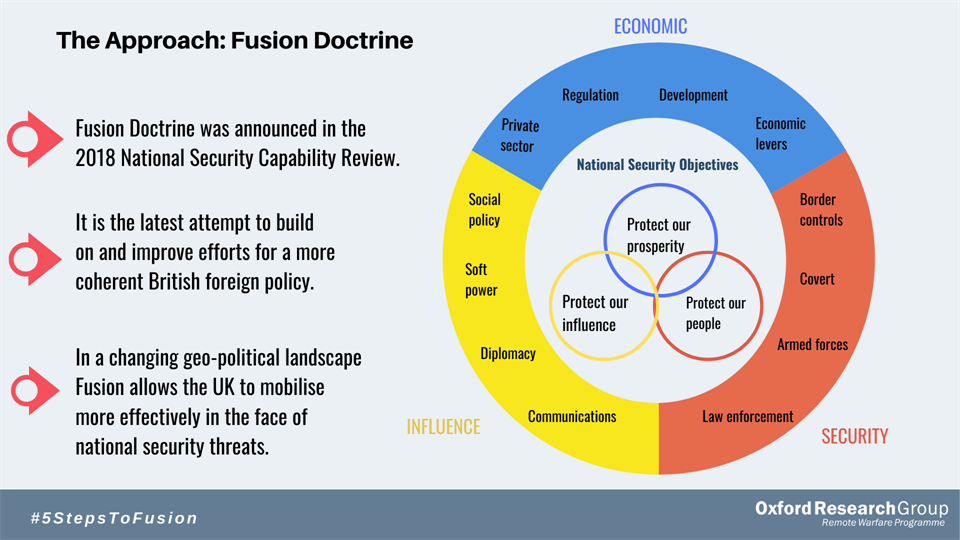
Source: Oxford Research Group
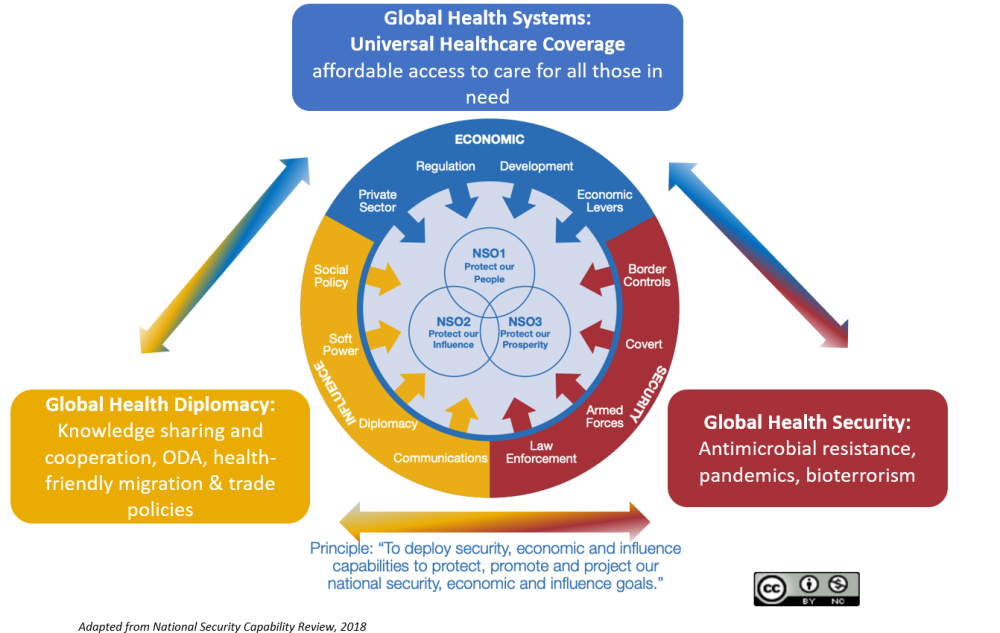
The UK has world-leading capabilities in public health, health research and innovation, health education, health services delivery, and military health. We believe these capabilities can make a critical contribution to the three national security objectives along the three core global health dimensions: global health security, global health diplomacy, and global health systems (see figure below). Perhaps, even less well-articulated as a proposition, the UK’s and other countries’ security sectors can also play a valuable role in strengthening health systems, especially in fragile states.
Below we outline how health could be included to support the national security objectives.
Global Health Security
Global health security is perhaps the best and easiest case to make for global health being a core component of a national security objective, and vice versa.
The COVID-19 outbreak is in progress, with cases and community transmission now recorded across all continents. Its impacts on health, security, and the global markets are far from known as the world braces for a pandemic. In parallel, several infectious disease outbreaks are ongoing in the poorest parts of the world, with (thankfully waning) Ebola in Eastern Congo, monkeypox in the DRC, cholera across Eastern Africa, and Lassa fever in Nigeria. The health, economic, and security impacts of antimicrobial resistance are also well documented (see here and here). Further, the UK’s Public Health Rapid Support Team recently deployed in Sierra Leone to establish cholera surveillance systems after severe flooding, and the UK’s Emergency Medical Team helped manage a diphtheria outbreak at a refugee camp in Bangladesh. The NHS and UK Defence Medical Services personnel provided emergency response for the Manchester arena bombing and the London terrorist attacks in 2017. The UK response to the Ebola outbreak in 2014 is another example of cross-government intervention in a health security emergency. These examples demonstrate UK capabilities for medical response in the wake of terrorist attacks or humanitarian emergencies.
But as the director of the African CDC recently said, “The global health chain is only as strong as its weakest link, so a disease threat anywhere can quickly become a threat everywhere.” As we have seen with Ebola, weak healthcare systems across Africa may well undermine global efforts to address current and future outbreaks, making investments in preparedness essential. Thus, a programmatic approach to using UK cross-government capabilities in support of global health security could reduce the impact of global health risks on the UK.
Global Health Diplomacy
The US Department of Health and Human Services, equivalent to the UK Department of Health and Social Care (DHSC), which has for the past two decades run an Office of Global Affairs, defines global health diplomacy as a means of “transcending diplomatic challenges and enabling the U.S. government to maintain strong and mutually beneficial ties to other countries [esp] in cases where more traditional diplomatic relationships may be strained." Similarly, the US Department of State runs an Office of Global Health Diplomacy headed by an ambassador-at-large (also in charge of PEPFAR and the US COVID-19 response). The UK’s track record is less consistent. The UK first published its “Health is Global” strategy in 2008, and it was reviewed in 2011, but not since then. It remained un- or underfunded and is presumably now expired.
Things changed with the recent boost in official development assistance (ODA) allocation to non-DFID departments including DHSC. DHSC’s ODA budget doubled between 2017 and 2018 to just under £200m, or 1.3 percent of the country’s aid budget—the highest it has ever been. DHSC is part of the cross-Whitehall Prosperity Fund (which has been not without challenges—e.g., see recent ICAI follow up review) and oversees the National Institute for Health Research ODA research allocation (again, with its own issues). In a timely update, the 2020 relaunch of the All-Party Parliamentary Group on Global Health’s review of the UK’s contribution to health globally includes several examples of how the UK’s NHS, academe, for-profit, and third sectors have influenced global health, current threats to this influence, and potential ways for enhancing the UK’s global health footprint (also discussed by one of us here and here). But it is hardly specific in terms of what to do next (nor was it meant to serve as an action plan), and the effort to date does not seem responsive to any whole-of government direction, leading to a series of fragmented and less well articulated initiatives in global health.
The integrated review offers an important opportunity to articulate the UK’s global health diplomacy objectives and relate these to the ODA allocations to DHSC and other Whitehall departments, so that the vision and direction of travel is clear to all, accountable leadership is defined, and criteria for success and its assessment is evident in the years to come.
Global Health Systems and UHC
As with the global health security and diplomacy agendas, influence, security, and prosperity all ultimately rely on strong, resilient health systems which meet the needs of their populations without impoverishing families or national treasuries, and without marginalising those in greatest need. This is where the UK’s contribution to health system strengthening—through multilateral and bilateral channels; through ODA targeted to countries directly; and through contributions to global public goods like disease and antimicrobial resistance surveillance and control, laboratory capacity and related actions—can make a difference. Global health is a major piece of UK development policy and spending; over a quarter of the 0.7 percent of GDP committed to aid is health related, with $1.3 billion channelled via DFID and another $633m through multilaterals (2017 data). Earlier this year DFID committed £1.5 billion to the Global Fund to Fight AIDS, TB and Malaria, making DFID one of three largest contributors after the US and France.
As we have argued before, the UK can support the global UHC agenda (and exert soft power) by supporting a better and fairer inward healthcare professional migration system (i.e., adopting the Global Skills Partnership); strengthening healthcare governance and priority-setting institutions, particularly critical in countries transitioning away from aid dependence; and encouraging the use of good-value, evidence-informed programmes, policies, and technological innovations at the global and national levels. The latter could be achieved by establishing a NICE for development (or at least global health) spending for UK and multilateral spend, and by boosting national capacities for such domestic institutions.
But we should not stop there; the fusion doctrine cannot but enforce the two-way relationship between health on one hand and security, influence, and prosperity, on the other. Below we posit that there is untapped potential in considering military health systems as potential conduits for strengthening civilian public health services striving to achieve UHC.
Military health as a vehicle for health system strengthening in fragile states
The security sector’s role in health systems has been overlooked as a component of a country’s health economy, despite its potential importance within health economies across the world. Military medical systems have often led organisational, professional, and clinical change in health systems (Florence Nightingale’s role in transforming nursing is a powerful example). There is clear historical and contemporary evidence of translating knowledge from military clinical sciences (such as preventive medicine, trauma care, mental health, and rehabilitation) into the civilian sector. Military medical systems are also an integral part of a nation’s crisis response system, usually providing the only deployable medical system under government control. Beyond conflict or complex emergencies, the security sector medical services can form a key component of medical sector reform. Indeed, it may be an important part of supporting national health sector development in areas such as emergency care, mental health, rehabilitation, HIV/AIDS control, tobacco control, and as part of a dialogue for chemical, biological, radiological, and nuclear arms control and peace.
Beyond the obvious relevance to the security objective, a number of nations use their military medical forces in support of ‘health diplomacy’ as a development tool with civil or military health services of partner nations. The US State Department has two long-standing programmes to build international peace-keeping capability, the Global Peace Operations Initiative and the African Peacekeeping Rapid Response Partnership. These are delivered as an integrated civil-military effort with partner states. China also has well-established civil-military fusion in health both nationally and as an international engagement tool. International bodies in civil-military co-ordination in regional crisis response are becoming more important. the North Atlantic Treaty Organisation (NATO) Joint Health Group of the Senior Civil Emergency Planning Committee (SCEPC) advise on the medical aspects of civil support for the Alliance ’s military operations or support for national authorities in civil emergencies. The United Nations Office for the Co-ordination of Humanitarian Affairs supports the Regional Consultative Group (RCG) on Humanitarian Civil-Military Coordination for Asia and the Pacific to enhance preparedness and cooperation in countries at a high risk of large-scale, sudden-onset disasters in which foreign military assets are likely to support an international response.
On a multilateral basis, there have been international partnerships in the security medical systems in Iraq through the NATO Training Mission Iraq, in Afghanistan during the NATO missions, and in Ukraine through the NATO’s Comprehensive Assistance Package for Ukraine and NATO runs a regional dialogue with neighbouring military medical services under the Partnership for Peace programme.
Finally, in most nations the armed forces have a medical system that provides health services support for deployed military operations. The armed forces health system—and other elements of the security sector health system—also provides community medical services for military personnel in garrisons (including primary care, dental care, rehabilitation, mental health and occupational health) and in many high-income and low- and middle-income countries, the security health sector provides a comprehensive range of health services for its beneficiaries (including all hospital specialties) as a parallel government service to the public health system. This makes access to the healthcare system a significant benefit of employment in the security sector and represents a substantial component of a country’s health economy.
As examples, in the US, the Departments of Defense and Veterans Affairs together provide healthcare for around 18.5 million beneficiaries, costing approximately $273bn, employing around 540,000 personnel, and managing some 221 hospitals and large health insurance schemes. In the UK, the dependant population of the Defence Medical Services is around 135,000, costing approximately £0.5bn and employing about 13,400 personnel, with no military hospitals. Jordan has a “militarised” Royal Medical Services that provides care for a third of the national population (2 million) through a network of 11 hospitals. Pakistan has 45 military hospitals and 34,200 personnel to care for around 7.4 million beneficiaries. In Nigeria, the needs of serving armed forces personnel, retirees, and their families are met by the nongovernment Defence Health Maintenance Limited though the 21 military hospitals and a network of affiliated civilian hospitals. The military systems in LMICs are oftentimes better resourced, attract high calibre and well-trained healthcare professionals, benefit from ICT systems, maintain a presence in remote rural areas, have a track record of clinical governance and audit and enjoy a reputation of better care quality and trust amongst the general population.
At the same time, such systems may be below capacity and inefficient, and may create inequitable access to clinical care for beneficiaries (in quality, access, or cost) compared to public health systems. Furthermore, clinical practice and research may lie outside civilian regulation or ethical control in areas such as biological research, care of prisoners, and confidentiality of medical information. If left outside the UHC discussion, the impact of such parallel “vertical” systems within fragile states in particular may remain neutral or crowd out their civilian counterparts. But if harnessed, the capacities of military medical systems could become a driver for UHC and a bridge for engaging through the British military medicine network, the latter well plugged into the UK’s publicly run NHS.
Conclusions
We call on the integrated review to consider health’s potential in serving the triple national security objectives of security (global health security), influence (global health diplomacy) and prosperity (global health systems and UHC), and also the relationships between defence and the military and global public health. Far from securitising global health, the 2020 integrated review can offer an alternative where the security infrastructure is placed at the service of strengthening fragile health systems to address shocks as diverse as pandemics, mass migration, simultaneous aid transitions or large numbers of people falling back into poverty due to catastrophic medical bills. Last year’s open letter by 141 generals calling on the US Congress and administration to protect and enhance the country’s budget for diplomacy and foreign aid, is a case in point.
In the weeks to come we will be convening together with our partners at Kings College London virtual and in person (virus permitting) exchanges to drive the discussion on the integrated review and the role of military health in the UHC agenda; watch this space!
Topics
CITATION
Chalkidou, Kalipso, Martin Bricknell, Richard Sullivan, Adrian Gheorghe, and Amanda Glassman. 2020. Why is Global Health Missing from the UK’s Integrated Review?. Center for Global Development.DISCLAIMER & PERMISSIONS
CGD's publications reflect the views of the authors, drawing on prior research and experience in their areas of expertise. CGD is a nonpartisan, independent organization and does not take institutional positions. You may use and disseminate CGD's publications under these conditions.




{kind=link}
{kind=link}