Recommended


Since its launch in November 2022, the Pandemic Fund, housed at the World Bank, has committed $885 million in grant financing to strengthen pandemic prevention, preparedness, and response (PPR) in developing countries. In December 2024, it invited new proposals for an additional $500 million in financing. With the recent mpox and Marburg outbreaks, and the growing frequency of such crises due to climate change, these funds are critical for bolstering global readiness. During its first call for proposals in March 2023, demand for Pandemic Fund financing exceeded supply by a staggering factor of 24.
Meanwhile, the International Monetary Fund (IMF) has a parallel resource—the Resilience and Sustainability Facility (RSF)—designed to provide long-term concessional financing to 143 countries, including all low-income countries, developing and vulnerable small states, and lower-middle-income countries. The RSF is designed to support both climate transition and pandemic preparedness, and since its lending operations began in October 2022, it has committed over $11 billion to 22 countries. However, while three countries have already completed their RSF programs, pandemic preparedness has not been included as a condition in any RSF program to date.
So, why the mismatch? Why is the Pandemic Fund oversubscribed while the RSF remains untapped for pandemic preparedness?
Previous blogs (here and here) have speculated about the reasons why countries have not sought RSF financing for pandemic preparedness. Possible explanations include the IMF staff’s lack of health policy expertise, insufficient collaboration between the IMF and institutions with health policy expertise, and a lack of interest from ministries of finance, which typically negotiate IMF programs, in addressing health concerns.
Given that RSF is significantly better funded than the Pandemic Fund, this discrepancy raises important questions. In this piece, we dive deeper into this puzzle—and suggest potential ways forward.
Revealed preference of countries tapping into the Pandemic Fund and RSF
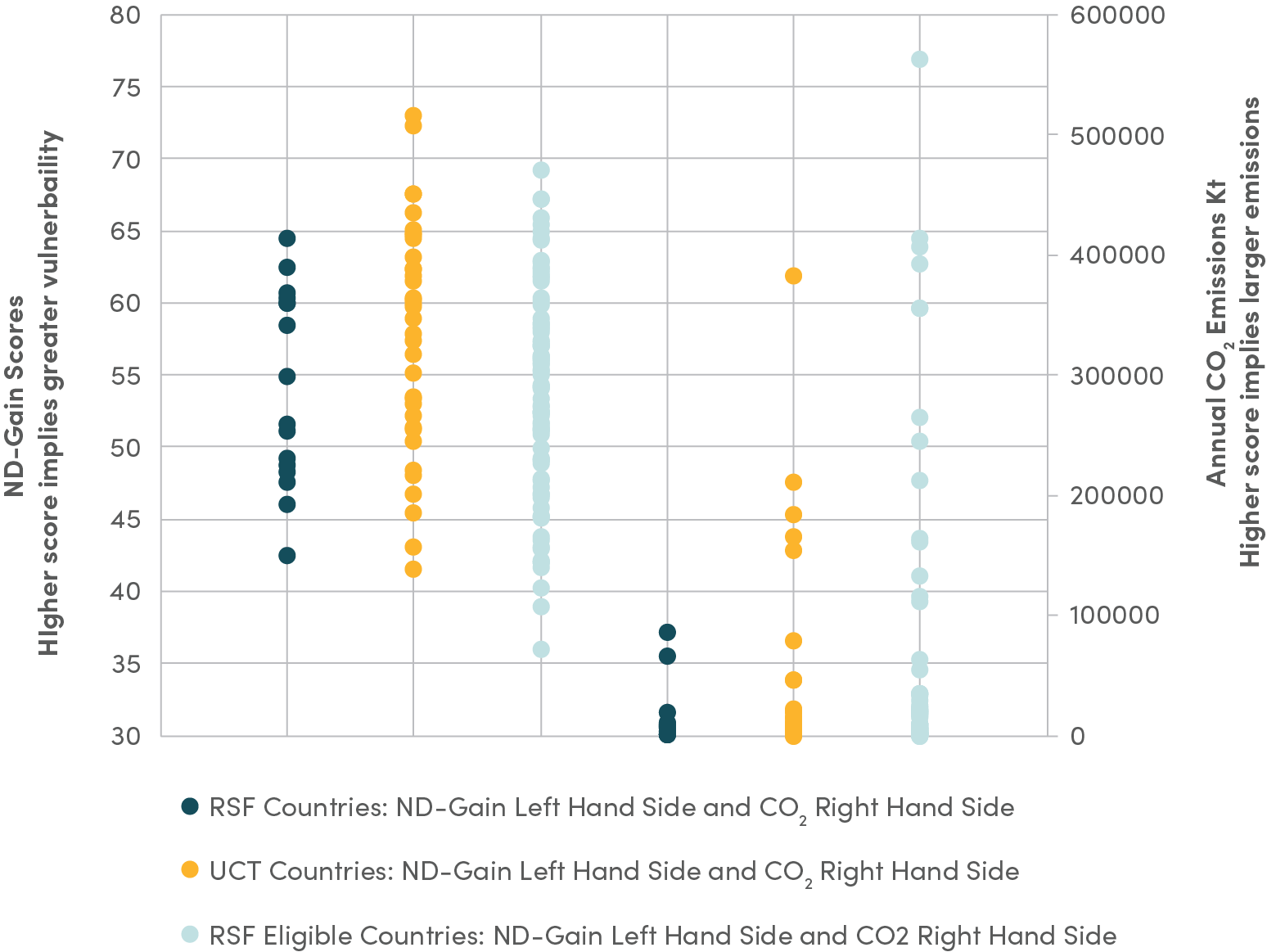
As Graphic 1 shows, 65 recipients of Pandemic Fund grant funding have not accessed financing from the RSF, despite the RSF’s significantly larger resources. These countries include Burundi and Uganda, both currently on the front lines of the mpox outbreak. On average, Pandemic Fund grant financing amounts to just $0.39 per capita (excluding co-financing and including multi-country projects*), an amount far too low to effectively support its three priority areas: strengthening surveillance systems, laboratory systems, and human resources. While the Pandemic Fund incorporates co-financing and co-investment mechanisms to attract additional resources from implementing entities, governmental donors, philanthropies, and the private sector, the inclusion of co-investment—primarily in-kind contributions from governments—may overestimate the actual financial resources available. Based on publicly-available estimates, this level of funding may only be sufficient to establish a basic surveillance system in a low- or lower-middle-income country—limiting the Pandemic Fund’s ability to fully deliver on its mandate.
Graphic 1. Countries that have taken funds from RSF, Pandemic Fund
*Includes all countries involved in multi-country projects.
In contrast, the RSF programs have committed $17.45 per capita to countries, which if spent even partially on PPR, could vastly expand the range and scale of PPR efforts. This level of financing is possible because the RSF offers financing of up to 150 percent of a country’s IMF quota or SDR 1 billion. While RSF funds are disbursed as loans, they come with highly concessional terms—20-year maturities and a 10.5-year grace period. Given this, it is striking that 65 countries that have actively sought PPR funding through the Pandemic Fund have not utilized the RSF for pandemic preparedness.
Table 1. Pandemic Fund, RST commitments
|
|
Total commitments |
Commitments per capita** |
||
|---|---|---|---|---|
|
Pandemic Fund |
$885 million |
$7.25 billion* |
$0.39 |
$4.25* |
|
RSF |
$11.2 billion |
$17.42 |
||
*Includes co-financing and co-investment.
**Based on recipient country populations using World Bank 2023 data.
Meanwhile, 10 countries—Bangladesh, Cabo Verde, the Democratic Republic of the Congo (DRC), Jamaica, Kenya, Madagascar, Moldova, Paraguay, Rwanda, and Tanzania—received both Pandemic Fund grant funding and RSF loans. Even in these cases, however, RSF programs did not include pandemic-related provisions. This disconnect may reflect both demand- and supply-side challenges, as previous CGD work has explored. On the demand-side, countries may prioritize climate finance over pandemic preparedness, particularly after elevated health spending during the COVID-19 pandemic. On the supply-side, the IMF has acknowledged a lack of expertise in pandemic preparedness and may prefer to focus on climate-related funding.
An additional factor that may explain this gap is the IMF’s requirement that countries have a concurrent upper credit tranche (UCT) program to access RSF financing. UCT programs, which involve loans exceeding 25 percent of a country’s quota, typically come with macroeconomic conditions. Of the 65 Pandemic Fund grant recipients that did not access RSF resources, only 19 have IMF programs that meet the UCT criterion. Of these, just 13 meet the RSF’s stipulation that the accompanying UCT program has 18 months remaining (though it could be a non-financing program, as was the case with Rwanda). This means that for 46 Pandemic Fund recipients, the UCT requirement is a barrier to RSF access.
The way forward
If the issue lies in a lack of health and pandemic expertise among IMF staff, strengthening collaboration between the Pandemic Fund, the IMF, and the World Health Organization (WHO) could provide a path forward. An interim review of the RSF in May 2024 highlighted key areas to help the facility achieve its intended objectives. The review acknowledged that RSF thus far had focused solely on climate-related challenges but would “soon include pandemic preparedness.” It noted growing interest from member countries in this shift and indicated that a cooperation framework with the World Bank and the WHO was being finalized to support its implementation.
After months of anticipation, the cooperation framework was released in early October 2024, outlining three “broad principles” for this collaboration. These principles focus on integrating pandemic risks into economic policy, leveraging WHO’s expertise to guide investments, and aligning financing strategies across institutions. However, despite this framework, the two countries approved for RSF since October 2024, Papua New Guinea and the DRC, have continued to focus exclusively on climate resilience, with no pandemic preparedness provisions included in their programs.
The DRC’s recent RSF arrangement underscores the missed opportunities in aligning RSF financing with pandemic preparedness. As the epicenter of mpox and a country frequently battling Ebola outbreaks, the DRC faces significant health challenges. In October 2024, it secured a $25 million project through the Pandemic Fund. However, integrating PPR conditions into its RSF program could have strengthened disease surveillance systems and public health infrastructure, delivering benefits for both the DRC and global health security. The absence of such conditions represents a missed opportunity, leaving the country—and the world—more vulnerable to future outbreaks.
Going forward, it is vital to focus RSF and Pandemic Fund resources on countries that are high-risk hotspots for infectious disease outbreaks. Nations like the DRC, which face recurring health crises, require targeted pandemic preparedness efforts. To achieve this, the RSF and the Pandemic Fund must work together to allocate resources more effectively to high-risk countries. Prioritizing hotspot countries aligns with the Pandemic Fund’s Results Framework, which emphasizes high-impact investments, while the RSF is uniquely positioned to amplify these efforts with its larger financial scale. Effective resource allocation should be guided by data, using epidemiological risk assessments and disease burden metrics to target countries and regions most in need.
The scheduled 2026 comprehensive review of the RSF presents a key opportunity to clarify the facility’s role in global health financing. If the RSF continues to exclude pandemic preparedness, the review should seriously consider removing this mandate from the facility. Alternatively, the review could serve as a chance to substantially expand, refine, and implement fit-for-purpose guidelines on World Bank-IMF-WHO collaboration. Enhanced collaboration, alongside some technical changes like the removing the UCT requirement for repeat borrowers or raising access limits for repeat borrowers to facilitate financing for pandemic preparedness, could enable the RSF to play a crucial role in strengthening countries’ health systems and support global public goods. By aligning the mandates, expertise, and financing capacities of the Pandemic Fund and the RSF, the global community can better prepare for future pandemics and reduce vulnerability to emerging infectious diseases.
Topics
DISCLAIMER & PERMISSIONS
CGD's publications reflect the views of the authors, drawing on prior research and experience in their areas of expertise. CGD is a nonpartisan, independent organization and does not take institutional positions. You may use and disseminate CGD's publications under these conditions.
Thumbnail image by: Media Lens King/ Adobe Stock



