Recommended

The IMF’s newly instituted Resilience and Sustainability Facility (RSF) has committed $7.4 billion to 20 low-income and emerging market countries to address challenges arising from climate change. The RSF was also intended to help countries prepare for pandemics, given the experiences of the COVID-19 pandemic and the economic scars it left behind. Indeed, the resources provided by the RSF come with highly concessional terms, repayable over 20 years with a grace period of 10.5 years.
Despite the recent declaration of the mpox public health emergency and recent release of the global strategic preparedness and response plan calling for $135 million to fund the plan, none of the 20 countries have sought RSF funding for pandemic preparedness. Donors and nations alike are expressing concern over the lack of resources allocated to the health sector in developing countries. In this piece, we explore possible reasons why countries are not utilizing the RSF for pandemic funding, including revealed preferences, implicit signaling, and interministerial dynamics. We conclude with broader challenges of global health financing architecture and the urgent need for a surge financing mechanism.
Is it “revealed preferences”?
The most obvious reason for the lack of take-up for pandemic-related funding from the RSF could be “revealed preference” by countries seeking RSF resources. In 2020, all countries increased their health spending in response to the COVID-19 pandemic by stretching their domestic budgets with additional support from donors. In low-income countries, domestic health spending increase averaged 0.3 percent of GDP, while in emerging economies, it was twice as much. The officials in these countries may believe that they have already dealt with one pandemic and, incorrectly, that the next one won't occur for some time. As a result, they may prefer to focus on other pressing issues, such as climate change—an area that requires huge investments going forward and has not benefited from the same level of concessional financing as the health sector (Figure 1).
Figure 1. Official development assistance for health, pandemics and climate
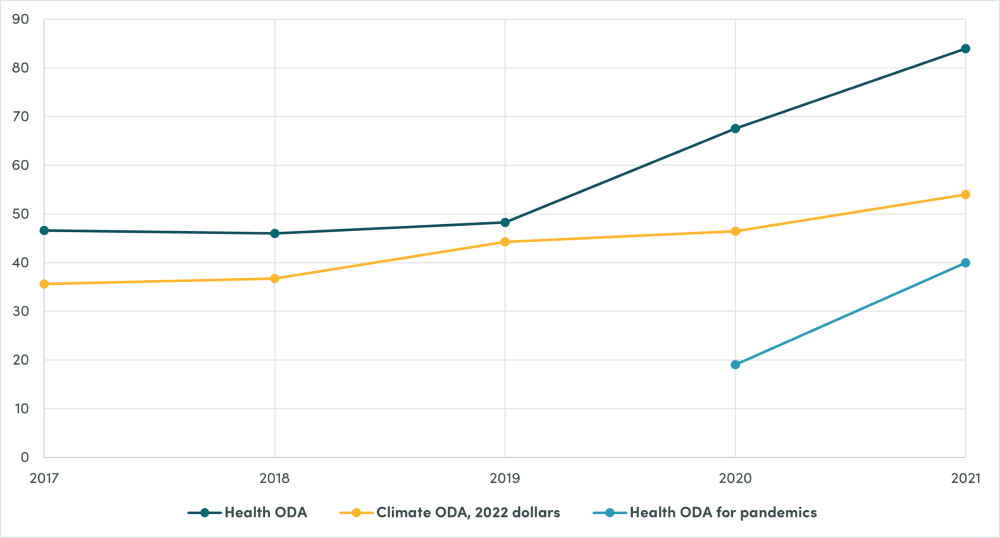
Source: Data for climate ODA are from OECD CRS: https://one.oecd.org/document/DCD(2024)20/en/pdf Data for health ODA are from IHME: http://ihmeuw.org/6g55 Figures are in 2022 US$ billions.
Is it because of IMF signaling?
Another plausible reason for the lack of take-up for pandemic funding under the RSF could be the signals the IMF is implicitly sending to countries. Even though the IMF offers RSF financing for both climate and pandemic preparedness, the implicit signals from the IMF may be steering countries towards climate-related funding. This bias might stem from the fact that IMF staff are generally better equipped to support climate initiatives, with many having developed expertise in the macroeconomic aspects of climate transition. On whole, these factors could be perceived by country authorities as an implicit nudge towards climate financing.
Moreover, the memorandum of understanding between the IMF, World Bank, and WHO on how to address pandemic preparedness within RSF programs has yet to be signed. Until collaboration is formalized, the tendency to prioritize climate over pandemic preparedness may continue.
The good news is that earlier this year, the IMF board reviewed the operations of the RSF and expressed interest in expanding the facility to include pandemic preparedness. They also requested more details on the IMF’s role in this area, particularly in comparison to institutions like the World Bank, WHO, and others.
Is it because of ministerial competition and “donor’s pet” dynamics
From the perspective of a health ministry in a developing country, the RSF may not be particularly attractive, especially when compared to grants from the Global Fund and IDA/IBRD (Figure 2).
Figure 2. Health aid disbursements of the Global Fund, IBRD, and IDA, 2013-22
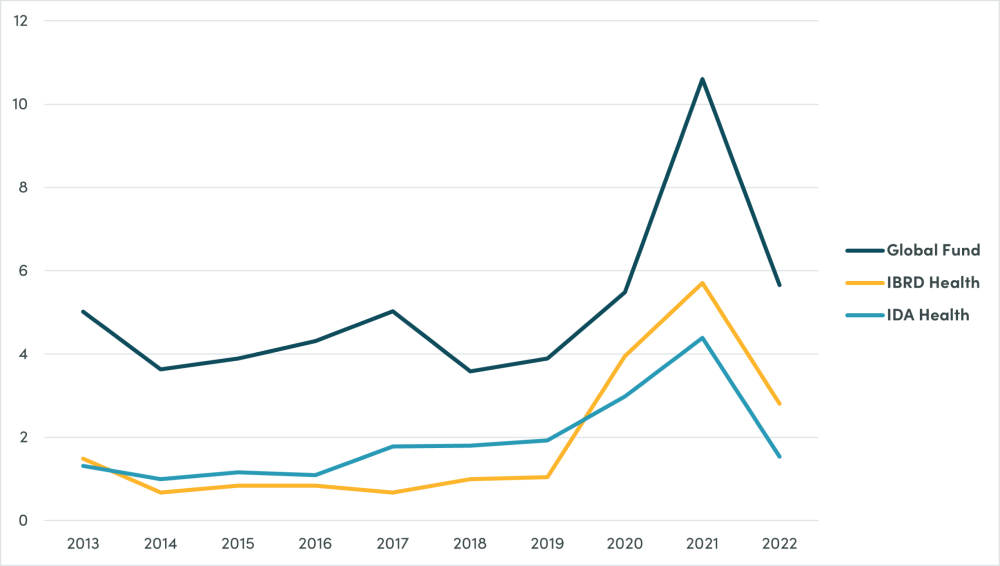
Source: Data are from IHME Financing Global Health database in 2022 US$ billions. The Global Fund refers to the Global Fund to Fight AIDS, Tuberculosis, and Malaria, three constitutive diseases and is used as an example of the off-budget grants model pervasive in global health.
Given a choice between grants and concessional loans, health ministries in developing countries might prefer the easier, more generous grant funding over concessional loans. Even though concessional loans are cheaper than market-rate loans, they are still costlier than grants, leaving health ministries with little incentive to consider funding sources that aren't pure grants. Besides, RSF conditionalities—many of which have tended to focus on strengthening public financial management—could lead to increased scrutiny from their finance ministry, particularly regarding budget execution and staffing vacancies. This potential for greater oversight may further discourage health ministries from seeking RSF resources
On the other hand, finance ministries, perhaps envious of the relatively abundant grant resources flowing into health—typically off-budget (i.e., off ministerial or government budgets)—might view the RSF as an opportunity to finally secure more funding for neglected areas like climate (as shown in Figure 1). While disbursements for IDA grants for all sectors exceeded that of Global Fund grants in 2022, this was not the case prior to 2018 (Figure 3). Finance ministries may also believe, not unlike donors, that a typical health ministry may lack the capacity to effectively manage and execute funds, especially after relying on off-budgetary grants for years, which in turn may have further weakened their operational capacities. This view is reinforced by consistent under-execution of budgets by several low-income developing countries.
Thus, it could be argued that the health sector is the “donor’s pet,” much like a “teacher pet,” receiving a disproportionate share of attention and resources. Other sectors not only see the disproportionate neglect in dollars, as illustrated in Figure 3 with $6.58 billion for all sector IDA grants compared to $5.3 billion for Global Fund in 2022. This sector has benefited from new buildings and vehicles, not to mention human resources, often in the form of incentives, per diems, and other benefits. During the pandemic, health priorities arguably further overshadowed other areas with negative consequences.
Given that the health sector is relatively better resourced compared to other sectors (and even within health, certain diseases are strongly prioritized over other diseases), it seems logical that finance ministries would prioritize other sectors, if only driven out of a sense of equity and fairness among ministries, thereby explaining the revealed preference for climate over pandemics under the RSF. These hypotheses also point to the need for greater engagement and better communication between ministries of finance and health, one of the justifications for the creation of the G20 Joint Finance and Health Taskforce.
Figure 3. Disbursements to all sectors from IDA loans and grants compared to Global Fund grants for its three constitutive diseases
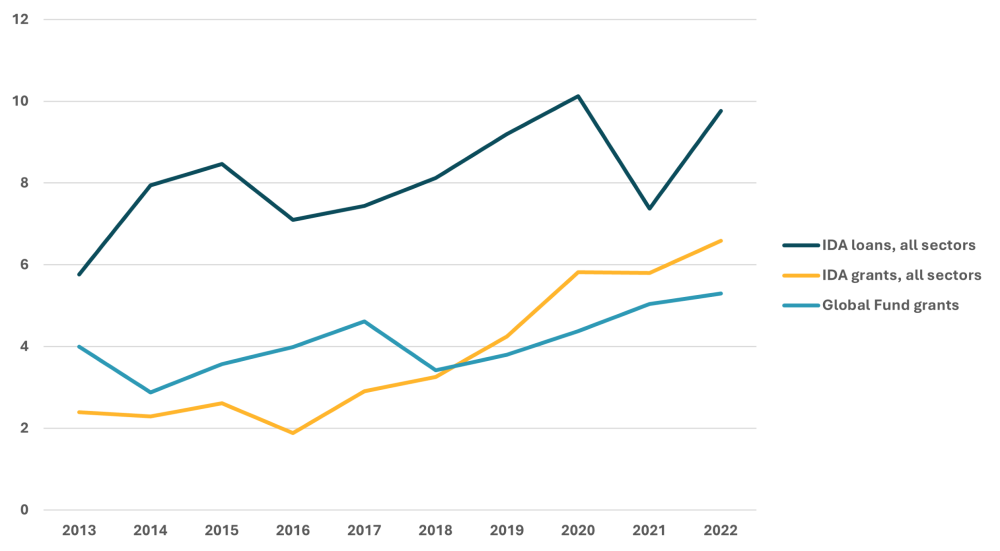
Source: OECD CRS for World Bank data and IHME for Global Fund data. The Global Fund refers to the Global Fund to Fight AIDS, Tuberculosis, and Malaria, three constitutive diseases and is used as an example of the off-budget grants model pervasive in global health.
Examine interministerial and donor dynamics
The hypotheses we’ve presented above highlight potential flaws in the current global health financing system more than the design of RSF.
While there is clear demand for more pandemic funding—as evidenced by the oversubscription to the Pandemic Fund of $5.5 billion requested compared to the $300 million available in the first call—this demand has not translated into requests for and take-up of RSF resources. This discrepancy warrants further investigation, including by the IMF. Some possible questions to explore are:
- What is happening in the RSF discussions between finance ministries and the IMF?
- What does insufficient attention to health compared to climate indicate about the IMF’s perceptions of the macroeconomic and fiscal implications of the health sector compared to climate?
We also note that the Pandemic Fund is not mandated to explore whether and how all possible funds, including from RSF and other donors, can be utilized for pandemic preparedness and response. But the Pandemic Fund can work with an individual country and development partners to finance preparedness and response plans and ensure that countries can tap into concessional resources such as the RSF.
Overall, the situation is less a mystery than a reflection of rational decision-making. Countries are simply making the best choices based on the options available, which may suggest a need for a broader reevaluation of how health assistance is structured.
Mpox pandemic déjà vu: who owns surge financing?
The mpox pandemic highlights a familiar issue: inadequate and slow surge financing. Even as the RSF is intended for preparedness rather than response, financing both preparedness and response arguably cannot be de-linked from each other. A newly released CGD and Disease Control Priorities (DCP) paper (coauthored by Fan, Kim, Pineda, and Berotzzi) reviewed pandemic financing across the cycles of prevention, preparedness, response, and recovery. The paper highlighted the sluggishness in response or surge financing and the continued lack of organizational home for such mechanism even now.
The policy community is grappling with questions of organizational design, not the forte of either economists or epidemiologists. Should the Pandemic Fund take on this role? Should we reimplement ACT-A or COVAX—effectively an ad hoc coordination structure—again? Are we going to wait for the new pandemic accord’s coordinated financial mechanism in two years? Should we leave it to the G7 development financial institutions (DFIs), who are advancing this issue but whose tools (non-concessional, small sums of money) address only part of the problem? Or is this like Waiting for Godot?
It is unclear what the official position of the Pandemic Fund is, or should be, about its role in the surge financing mechanism. Certainly, in its inaugural year, the Pandemic Fund faced significant challenges financing preparedness, with minimal resources in its first tranche. Perhaps they opted to avoid response financing to maintain focus, understandable in the short term. Including response financing into the Pandemic Fund’s mandate may risk diluting its core focus on preparedness—also understandable given the well-known fact that treatment (and response) tends to crowd out public health (including prevention and preparedness) in line-item budgets, unless there are protected line items in the budget.
Yet its name is all-encompassing, suggestive of the entire pandemic cycle, and with no other entity with such a comprehensive name. Thus, the Pandemic Fund is ostensibly responsible for addressing pandemic financing. After the World Bank closed its Pandemic Emergency Financing Facility, the world lost its one response financing mechanism, however poorly designed and with no immediate replacement or successor. So if the Pandemic Fund does not take ownership of response financing, it’s unclear who will.
We could face another confused, chaotic, and incredibly slow response to mpox in 2024. Alternatively, entities like Gavi’s First Response Fund and Global Fund might tap into their funds that drew on reallocated COVAX funds for pandemic response and assert their leadership in the absence of clear ownership. Meanwhile, WHO will likely continue its model as one focuses on technical assistance through staffing, rather a financing or disbursement model for which Gavi, the Global Fund, and the multilateral development banks are known. Indeed, the newly released WHO Strategic Preparedness and Response Plan calls for a “financing coordination mechanism” to be “implemented (by) donors and financing institutions to mobilize and allocate resources” (see page 15 in the document).
The CGD-DCP pandemic financing paper argued that incentives for both preparedness and response are crucial and linked to each other. This may be the strongest argument for why the Pandemic Fund should encompass both.
With thanks to discussions with Masood Ahmed, Victoria Dimond, Nancy Lee, and various colleagues.
Topics
DISCLAIMER & PERMISSIONS
CGD's publications reflect the views of the authors, drawing on prior research and experience in their areas of expertise. CGD is a nonpartisan, independent organization and does not take institutional positions. You may use and disseminate CGD's publications under these conditions.
Thumbnail image by: IMF Photo/Esther Ruth Mbabazi



